Tuberculosis is a contagious bacterial infection primarily affecting the lungs but can spread to other organs, causing severe health complications if untreated. Early detection and consistent treatment with prescribed antibiotics are crucial to prevent resistance and transmission. Discover how you can recognize symptoms, understand treatments, and protect yourself by reading the rest of this article.
Table of Comparison
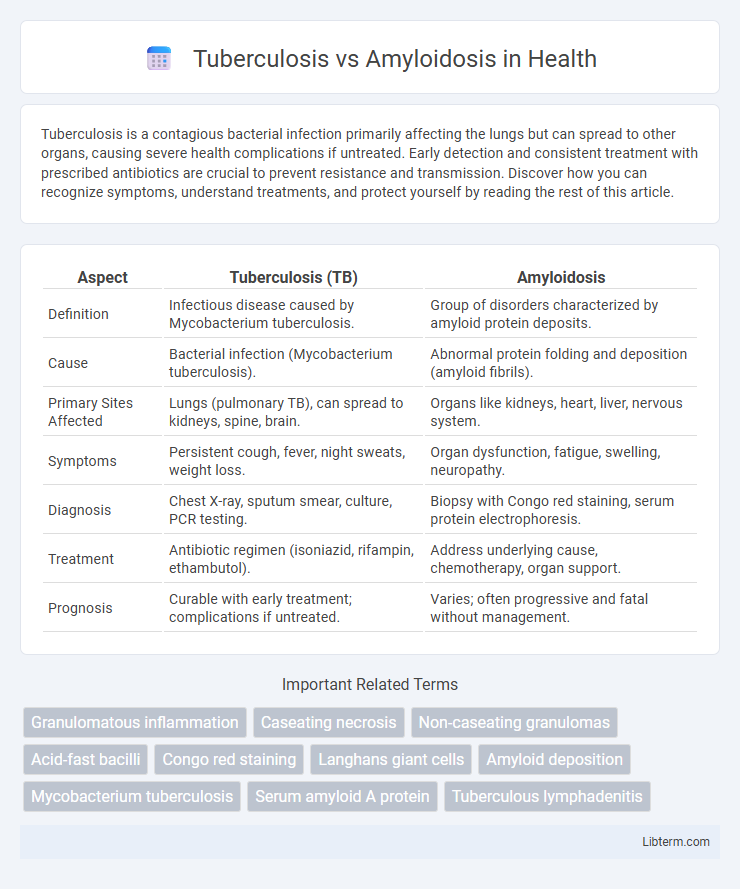
| Aspect | Tuberculosis (TB) | Amyloidosis |
|---|---|---|
| Definition | Infectious disease caused by Mycobacterium tuberculosis. | Group of disorders characterized by amyloid protein deposits. |
| Cause | Bacterial infection (Mycobacterium tuberculosis). | Abnormal protein folding and deposition (amyloid fibrils). |
| Primary Sites Affected | Lungs (pulmonary TB), can spread to kidneys, spine, brain. | Organs like kidneys, heart, liver, nervous system. |
| Symptoms | Persistent cough, fever, night sweats, weight loss. | Organ dysfunction, fatigue, swelling, neuropathy. |
| Diagnosis | Chest X-ray, sputum smear, culture, PCR testing. | Biopsy with Congo red staining, serum protein electrophoresis. |
| Treatment | Antibiotic regimen (isoniazid, rifampin, ethambutol). | Address underlying cause, chemotherapy, organ support. |
| Prognosis | Curable with early treatment; complications if untreated. | Varies; often progressive and fatal without management. |
Introduction to Tuberculosis and Amyloidosis
Tuberculosis (TB) is an infectious disease caused by the bacterium Mycobacterium tuberculosis, primarily affecting the lungs but capable of spreading to other organs. Amyloidosis is a rare disorder characterized by abnormal deposition of amyloid proteins in tissues and organs, leading to organ dysfunction and systemic complications. Differentiating between TB and amyloidosis is critical due to their distinct etiologies, pathophysiologies, and treatment approaches.
Understanding Tuberculosis: Causes and Transmission
Tuberculosis is a contagious bacterial infection caused by Mycobacterium tuberculosis, primarily transmitted through airborne droplets from coughs or sneezes of an infected person. It primarily affects the lungs but can spread to other organs, causing symptoms like persistent cough, weight loss, fever, and night sweats. Understanding the mode of transmission and risk factors such as close contact with infected individuals and weakened immune systems is crucial for preventing the spread of tuberculosis.
Amyloidosis: Definition and Disease Mechanism
Amyloidosis is a group of diseases characterized by the abnormal deposition of amyloid proteins in tissues and organs, disrupting their normal function. The disease mechanism involves misfolded protein precursors aggregating into insoluble fibrils that accumulate extracellularly, leading to organ dysfunction and damage. This pathological protein aggregation distinguishes amyloidosis from Tuberculosis, which is caused by Mycobacterium tuberculosis infection.
Key Differences in Pathophysiology
Tuberculosis is caused by Mycobacterium tuberculosis infection leading to granulomatous inflammation characterized by caseating necrosis, whereas amyloidosis results from extracellular deposition of insoluble amyloid fibrils disrupting normal tissue architecture. In tuberculosis, immune response triggers macrophage activation and formation of granulomas aimed at containing the bacteria, while amyloidosis involves abnormal protein folding and accumulation affecting organ function. Tuberculosis primarily affects the lungs and can cause chronic inflammation, whereas amyloidosis targets multiple organs, causing progressive organ failure due to fibril deposition.
Clinical Manifestations: Symptoms Comparison
Tuberculosis primarily presents with chronic cough, hemoptysis, fever, night sweats, weight loss, and fatigue, often indicating pulmonary involvement. Amyloidosis manifests with diverse symptoms depending on organ involvement, including nephrotic syndrome, restrictive cardiomyopathy, hepatomegaly, and peripheral neuropathy, reflecting systemic amyloid deposition. While tuberculosis symptoms are largely infectious and respiratory, amyloidosis symptoms arise from multi-organ dysfunction due to extracellular protein accumulation.
Diagnostic Approaches for Tuberculosis and Amyloidosis
Diagnostic approaches for Tuberculosis primarily include sputum smear microscopy, culture tests, and molecular methods like PCR to detect Mycobacterium tuberculosis DNA, alongside chest X-rays to visualize lung involvement. Amyloidosis diagnosis relies on tissue biopsy stained with Congo red to reveal amyloid deposits, supported by serum and urine protein electrophoresis to identify abnormal protein precursors, and advanced imaging such as cardiac MRI for organ-specific amyloid detection. Both conditions require specific biomarkers and imaging to accurately distinguish their pathophysiological manifestations and guide targeted treatment strategies.
Risk Factors and Populations Affected
Tuberculosis primarily affects populations with weakened immune systems, including those with HIV/AIDS, malnutrition, and crowded living conditions, posing a significant risk in low-income regions with limited healthcare access. Amyloidosis risk factors include chronic inflammatory diseases, genetic predisposition, and advanced age, predominantly impacting middle-aged to elderly individuals in developed countries where chronic illness prevalence is higher. Both diseases disproportionately affect vulnerable groups but differ in underlying causes and demographic distribution.
Treatment Modalities: TB vs. Amyloidosis
Treatment modalities for Tuberculosis primarily involve a combination of first-line antibiotics such as isoniazid, rifampin, ethambutol, and pyrazinamide over a 6-month course to eradicate Mycobacterium tuberculosis. Amyloidosis treatment focuses on reducing amyloid protein production using chemotherapy agents like melphalan and dexamethasone or targeted therapies, alongside supportive care for organ dysfunction. Management of TB requires strict adherence to antimicrobial therapy to prevent resistance, whereas amyloidosis treatment emphasizes controlling the underlying plasma cell disorder or chronic inflammatory disease driving amyloid deposition.
Complications and Prognostic Outcomes
Tuberculosis can lead to severe complications such as pulmonary fibrosis, respiratory failure, and dissemination to organs causing miliary tuberculosis, which significantly worsens prognosis with potential mortality if untreated. Amyloidosis primarily results in organ dysfunction due to amyloid protein deposits, causing heart failure, nephrotic syndrome, and neuropathy, with prognosis depending on amyloid type and affected organs. Both diseases carry high morbidity, but amyloidosis generally has a poorer long-term prognosis due to irreversible organ damage, while tuberculosis outcomes improve markedly with timely antimicrobial therapy.
Prevention and Public Health Strategies
Preventing tuberculosis relies heavily on widespread vaccination with the Bacillus Calmette-Guerin (BCG) vaccine, early detection through screening programs, and ensuring proper treatment adherence to reduce transmission and drug resistance. Amyloidosis prevention focuses on managing underlying conditions such as chronic infections and inflammatory diseases, with no direct vaccine available; public health efforts emphasize early diagnosis and controlling contributing factors to limit disease progression. Both diseases demand robust public health infrastructure, including awareness campaigns, healthcare access, and surveillance systems to mitigate impact on vulnerable populations.
Tuberculosis Infographic