Spasticity is a condition characterized by abnormal muscle tightness due to prolonged muscle contraction, commonly resulting from neurological disorders such as cerebral palsy, multiple sclerosis, or stroke. Effective management often involves physical therapy, medications, and in some cases, surgical interventions to improve mobility and reduce discomfort. Explore the rest of this article to understand how spasticity can impact your daily life and the latest treatment options available.
Table of Comparison
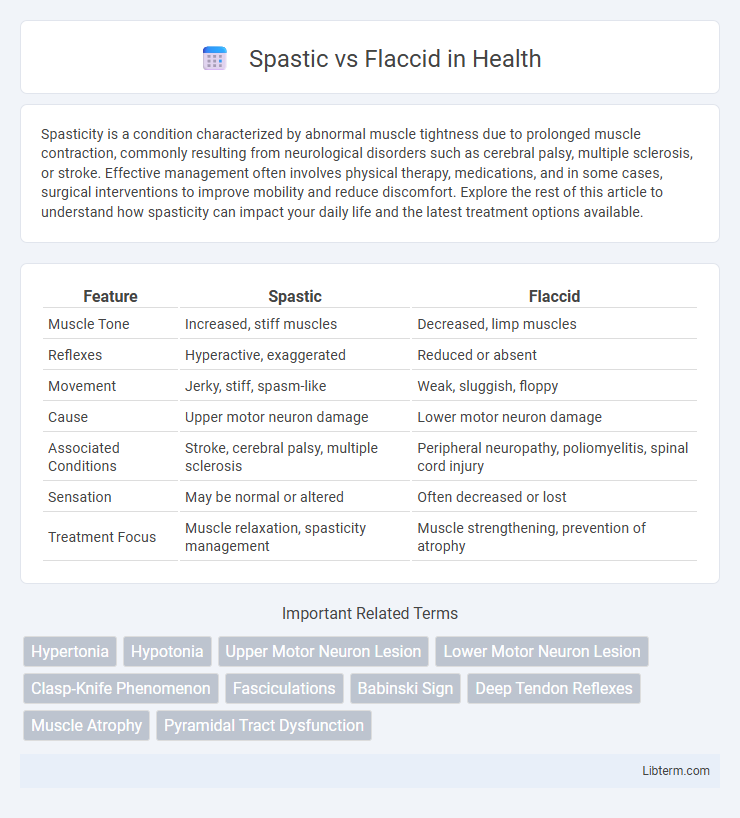
| Feature | Spastic | Flaccid |
|---|---|---|
| Muscle Tone | Increased, stiff muscles | Decreased, limp muscles |
| Reflexes | Hyperactive, exaggerated | Reduced or absent |
| Movement | Jerky, stiff, spasm-like | Weak, sluggish, floppy |
| Cause | Upper motor neuron damage | Lower motor neuron damage |
| Associated Conditions | Stroke, cerebral palsy, multiple sclerosis | Peripheral neuropathy, poliomyelitis, spinal cord injury |
| Sensation | May be normal or altered | Often decreased or lost |
| Treatment Focus | Muscle relaxation, spasticity management | Muscle strengthening, prevention of atrophy |
Understanding Spastic and Flaccid Conditions
Spastic and flaccid conditions represent two distinct types of muscle tone abnormalities often resulting from neurological disorders. Spasticity involves increased muscle tone leading to stiffness and exaggerated reflexes, commonly seen in conditions like cerebral palsy and stroke. Flaccid paralysis is characterized by decreased muscle tone and weakness, resulting in limp muscles and reduced reflexes, frequently associated with peripheral nerve injuries or spinal cord damage.
Key Differences Between Spastic and Flaccid Types
Spastic and flaccid are two distinct types of muscle tone disorders characterized by opposite symptoms; spasticity involves increased muscle tone leading to stiffness and exaggerated reflexes, whereas flaccidity results in decreased muscle tone causing weakness and limpness. Spastic muscles resist passive movement due to hyperactive stretch reflexes, while flaccid muscles lack resistance, often indicating damage to lower motor neurons or peripheral nerves. Understanding these key differences is crucial for accurate diagnosis and targeted rehabilitation strategies in neurological conditions such as cerebral palsy, stroke, or spinal cord injury.
Causes of Spasticity
Spasticity primarily results from damage to the upper motor neurons in the brain or spinal cord, commonly caused by conditions such as stroke, cerebral palsy, multiple sclerosis, and traumatic brain or spinal injuries. This neural impairment disrupts the balance of excitatory and inhibitory signals, leading to increased muscle tone and exaggerated reflexes characteristic of spasticity. In contrast, flaccid paralysis stems from lower motor neuron lesions, causing muscle weakness and decreased tone without reflex hyperactivity.
Causes of Flaccidity
Flaccidity, characterized by decreased muscle tone and weakness, primarily results from lower motor neuron lesions affecting the spinal cord, peripheral nerves, or muscle fibers. Common causes include peripheral nerve injury, poliomyelitis, Guillain-Barre syndrome, and muscular dystrophies leading to disrupted neuromuscular transmission. Unlike spasticity, which stems from upper motor neuron damage, flaccidity arises due to direct damage to the motor units responsible for voluntary muscle contraction.
Symptoms: Spastic vs Flaccid Presentation
Spastic presentation is characterized by increased muscle tone, hyperreflexia, and muscle stiffness, often resulting in jerky or exaggerated movements. Flaccid presentation involves decreased muscle tone, muscle weakness, and diminished or absent reflexes, causing limp and floppy limbs. Distinguishing these symptoms is crucial for diagnosing underlying neurological disorders such as upper motor neuron lesions in spasticity and lower motor neuron lesions in flaccidity.
Diagnostic Approaches
Diagnostic approaches for spastic and flaccid conditions primarily involve clinical examination and neurophysiological tests to distinguish muscle tone abnormalities. Spasticity is identified through increased muscle tone, hyperreflexia, and resistance to passive movement, often confirmed by electromyography (EMG) showing continuous motor unit activity. Flaccidity presents with decreased muscle tone, muscle weakness, and diminished or absent reflexes, with nerve conduction studies helping to pinpoint peripheral nerve or lower motor neuron involvement.
Effects on Muscle Function
Spastic muscles exhibit increased tone and stiffness due to hyperactive stretch reflexes, resulting in reduced voluntary control and difficulty with precise movements. Flaccid muscles, in contrast, show decreased tone, weakness, and diminished reflexes, often causing muscle atrophy and loss of movement. Both conditions disrupt normal muscle function but differ fundamentally in their neurological causes and clinical presentations.
Treatment Options for Spasticity and Flaccidity
Treatment options for spasticity include physical therapy, oral medications like baclofen and tizanidine, and intrathecal baclofen pumps to reduce muscle stiffness. Flaccidity management involves physical therapy to improve muscle tone and electrical stimulation to enhance muscle activation. In severe cases of spasticity, botulinum toxin injections are used to target specific muscles, while flaccid muscles may benefit from orthopedic interventions and assistive devices.
Rehabilitation and Therapy Strategies
Spastic and flaccid paralysis require distinct rehabilitation and therapy strategies targeting muscle tone abnormalities and motor function recovery. Spastic paralysis therapy emphasizes stretching, strengthening, and neuromuscular re-education to reduce hypertonia and improve voluntary movement, while flaccid paralysis rehabilitation focuses on preventing muscle atrophy through passive range-of-motion exercises, electrical stimulation, and functional training. Effective management employs tailored physical and occupational therapy programs, incorporating assistive devices and biofeedback to enhance neural plasticity and optimize functional independence.
Prognosis and Long-Term Outcomes
Spastic paralysis often results from upper motor neuron damage, leading to increased muscle tone and stiffness, with prognosis dependent on the severity and location of the injury, where some patients experience partial recovery through rehabilitation. Flaccid paralysis arises from lower motor neuron lesions causing muscle weakness and decreased tone, typically associated with a poorer prognosis due to irreversible nerve damage. Long-term outcomes in spastic paralysis may include improved motor function and managed spasticity, while flaccid paralysis frequently results in permanent muscle atrophy and limited functional recovery.
Spastic Infographic