Proliferative refers to the rapid growth or increase of cells, tissues, or structures, often seen in medical conditions such as proliferative diabetic retinopathy and proliferative lupus nephritis. Understanding the mechanisms behind proliferative processes is crucial for diagnosis, treatment, and monitoring disease progression to improve health outcomes. Discover more about how proliferative changes impact your well-being and the latest therapeutic approaches by reading the rest of this article.
Table of Comparison
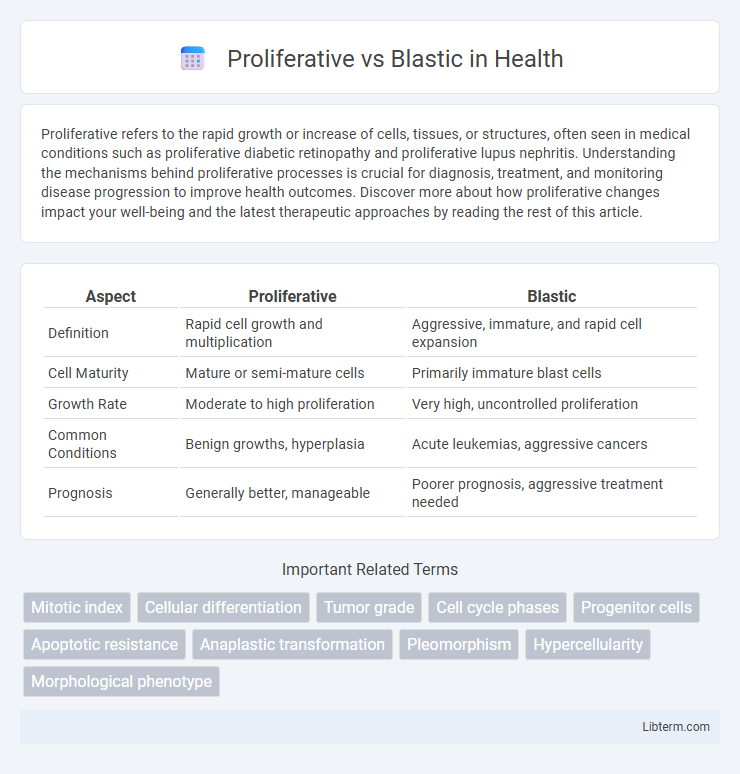
| Aspect | Proliferative | Blastic |
|---|---|---|
| Definition | Rapid cell growth and multiplication | Aggressive, immature, and rapid cell expansion |
| Cell Maturity | Mature or semi-mature cells | Primarily immature blast cells |
| Growth Rate | Moderate to high proliferation | Very high, uncontrolled proliferation |
| Common Conditions | Benign growths, hyperplasia | Acute leukemias, aggressive cancers |
| Prognosis | Generally better, manageable | Poorer prognosis, aggressive treatment needed |
Understanding Proliferative and Blastic Disorders
Proliferative and blastic disorders both involve abnormal cell growth but differ in their cellular characteristics and clinical implications. Proliferative disorders are marked by excessive multiplication of mature cells, leading to tissue enlargement or organ dysfunction, while blastic disorders feature an accumulation of immature precursor cells or blasts, often indicating aggressive malignancies such as acute leukemias. Understanding the distinctions between these disorders is crucial for accurate diagnosis, prognosis, and targeted treatment strategies in hematology and oncology.
Defining Proliferative Lesions
Proliferative lesions are characterized by an increase in cell division and tissue growth, often resulting in the expansion of normal or abnormal cells within an organ or tissue. These lesions can be benign or malignant, with proliferative activity indicating active cellular replication but not necessarily aggressive behavior. Understanding proliferative lesions is critical in distinguishing them from blastic lesions, which typically involve the production of immature precursor cells or blasts, often seen in hematologic malignancies like leukemia.
Key Characteristics of Blastic Lesions
Blastic lesions are characterized by the rapid and abnormal proliferation of immature precursor cells, often leading to aggressive tumor growth and poor differentiation. These lesions typically exhibit high mitotic activity, a dense cellular architecture, and a predilection for bone formation or sclerosis. Distinct from proliferative lesions, blastic lesions demonstrate marked cellular atypia and a strong potential for malignancy, frequently associated with hematologic cancers such as acute leukemia or blastic plasmacytoid dendritic cell neoplasm.
Cellular Pathways in Proliferation vs Blastic Activity
Proliferative activity primarily involves cellular pathways such as the PI3K/AKT/mTOR and MAPK/ERK cascades, which drive cell cycle progression and DNA replication. In contrast, blastic activity is characterized by altered differentiation pathways, including dysregulated Wnt/b-catenin and Notch signaling, promoting the accumulation of immature precursor cells. The differential engagement of these pathways defines the aggressive growth in proliferative states versus the arrested maturation seen in blastic conditions.
Diagnostic Criteria for Proliferative Conditions
Proliferative conditions are characterized by increased cellular growth with organized tissue architecture, whereas blastic conditions exhibit immature, poorly differentiated cells. Diagnostic criteria for proliferative disorders include histopathological evidence of hyperplasia, increased mitotic activity, and preservation of normal cellular differentiation patterns. Immunohistochemical markers such as Ki-67 help quantify proliferation rates, aiding differential diagnosis from blastic neoplasms.
Radiologic Features: Proliferative vs Blastic
Proliferative radiologic features typically include mixed lytic and sclerotic lesions with ill-defined margins indicating active bone turnover, whereas blastic lesions present as predominantly dense, sclerotic areas with well-demarcated borders reflecting increased bone formation. Proliferative patterns often correlate with aggressive tumor growth and destruction on imaging modalities such as MRI and CT scans, contrasting with blastic patterns that show homogeneous hyperdensity on X-rays and reduced marrow space. Recognizing the distinction between proliferative and blastic radiologic features aids in diagnosing the nature of bone pathology and assessing treatment response.
Clinical Manifestations: Differentiating Features
Proliferative and blastic lesions present distinct clinical manifestations critical for differential diagnosis; proliferative lesions typically exhibit gradual tissue expansion with mild symptoms, while blastic lesions often cause aggressive bone formation associated with pain and swelling. Proliferative conditions may show localized functional impairment without systemic signs, whereas blastic lesions frequently correlate with systemic symptoms such as fever and malaise due to their aggressive pathology. Imaging features like increased bone density in blastic lesions contrast with soft tissue proliferation seen in proliferative types, aiding in clinical differentiation.
Common Diseases Associated with Proliferative Patterns
Proliferative patterns are commonly associated with diseases such as proliferative glomerulonephritis, lupus nephritis, and diabetic nephropathy, where abnormal cell proliferation leads to inflammation and tissue damage. These conditions often show increased mesangial and endothelial cell proliferation, resulting in thickened capillary walls and reduced kidney function. In contrast, blastic patterns are mainly linked to acute leukemia types characterized by immature blast cells.
Diseases Frequently Presenting with Blastic Lesions
Blastic lesions are commonly associated with diseases such as multiple myeloma, metastatic prostate cancer, and osteosarcoma, where abnormal new bone formation is a hallmark. These lesions contrast with proliferative lesions, which emphasize increased cellular growth without necessarily causing new bone production. Identifying blastic lesions through imaging and biopsy aids in diagnosing these malignancies and tailoring appropriate treatment strategies.
Therapeutic Implications and Prognosis
Proliferative and blastic phases in hematologic malignancies exhibit distinct cellular behavior impacting therapeutic strategies and prognosis. Proliferative phases often respond better to cytoreductive therapies aimed at controlling cell growth, while blastic phases require aggressive chemotherapy due to rapid accumulation of immature blast cells. Prognosis worsens significantly in blastic phases due to higher resistance to treatment and increased risk of disease progression or relapse.
Proliferative Infographic