Mechanical methods such as the Foley catheter provide a reliable technique for cervical ripening by applying direct pressure to the cervix, stimulating dilation without the use of medications. This approach minimizes risks associated with pharmacologic agents, making it a preferred choice in certain clinical scenarios. Explore the full article to understand how you can benefit from mechanical methods during labor induction.
Table of Comparison
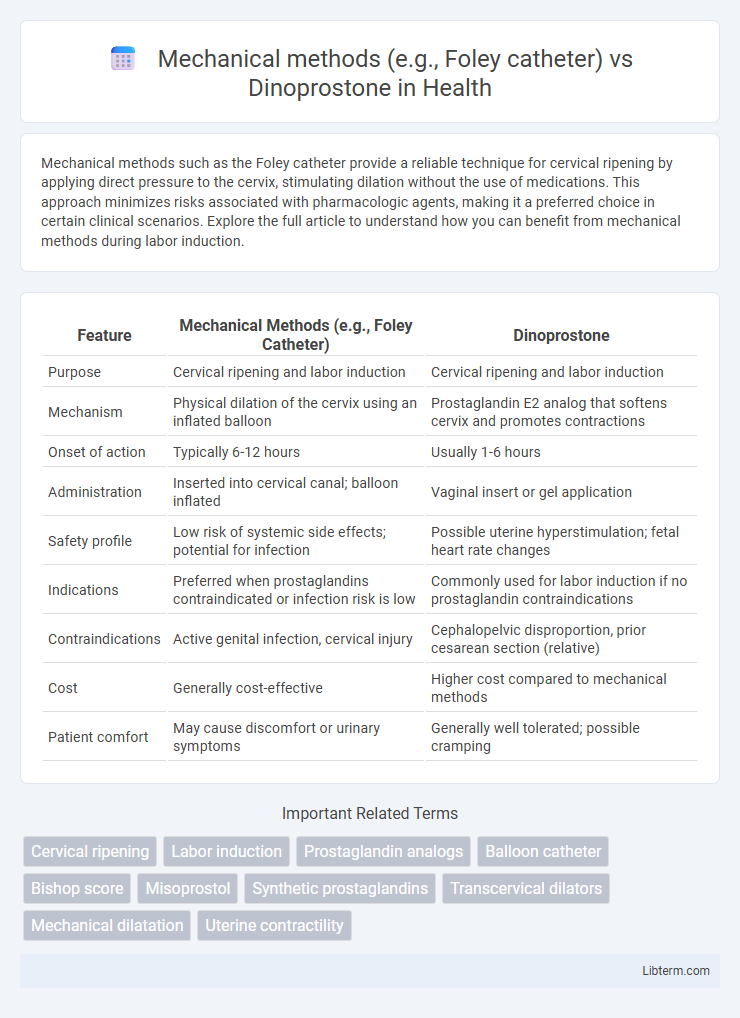
| Feature | Mechanical Methods (e.g., Foley Catheter) | Dinoprostone |
|---|---|---|
| Purpose | Cervical ripening and labor induction | Cervical ripening and labor induction |
| Mechanism | Physical dilation of the cervix using an inflated balloon | Prostaglandin E2 analog that softens cervix and promotes contractions |
| Onset of action | Typically 6-12 hours | Usually 1-6 hours |
| Administration | Inserted into cervical canal; balloon inflated | Vaginal insert or gel application |
| Safety profile | Low risk of systemic side effects; potential for infection | Possible uterine hyperstimulation; fetal heart rate changes |
| Indications | Preferred when prostaglandins contraindicated or infection risk is low | Commonly used for labor induction if no prostaglandin contraindications |
| Contraindications | Active genital infection, cervical injury | Cephalopelvic disproportion, prior cesarean section (relative) |
| Cost | Generally cost-effective | Higher cost compared to mechanical methods |
| Patient comfort | May cause discomfort or urinary symptoms | Generally well tolerated; possible cramping |
Introduction to Cervical Ripening Methods
Mechanical methods such as Foley catheters promote cervical ripening by applying direct pressure on the cervix, leading to endogenous prostaglandin release and gradual dilation. Dinoprostone, a synthetic prostaglandin E2 analogue, chemically induces cervical softening and uterine contractions by stimulating prostaglandin receptors. Both approaches aim to facilitate labor induction but differ fundamentally in their mechanisms, efficacy profiles, and side effect spectra.
Overview of Mechanical Methods: Foley Catheter
Foley catheter, a common mechanical method for cervical ripening, involves inserting a balloon catheter into the cervix and inflating it to apply pressure, promoting dilation through direct physical stimulation. This technique is associated with reduced risks of uterine hyperstimulation compared to pharmacological agents like dinoprostone, which chemically induce contractions. Mechanical methods such as the Foley catheter are favored in cases where minimizing systemic side effects is crucial, offering effective cervical ripening while maintaining a lower incidence of adverse maternal and fetal outcomes.
Understanding Dinoprostone: Pharmacological Approach
Dinoprostone, a synthetic prostaglandin E2, induces cervical ripening by softening the cervix and stimulating uterine contractions through its action on prostaglandin receptors, thereby facilitating labor onset. Unlike mechanical methods such as Foley catheter insertion, which physically dilate the cervix, Dinoprostone acts pharmacologically to promote biochemical changes in cervical tissue, improving its readiness for labor. Its precise dosing and controlled release formulation enhance efficacy and safety, reducing the risk of hyperstimulation compared to mechanical induction methods.
Mechanism of Action: Mechanical vs. Pharmacologic
Mechanical methods like the Foley catheter induce cervical ripening by physically dilating the cervix, exerting direct pressure on the cervical canal to promote endogenous prostaglandin release and stimulate labor. Dinoprostone, a synthetic prostaglandin E2, acts pharmacologically by binding to prostaglandin receptors in the cervix and uterus, leading to biochemical softening of cervical collagen and induction of uterine contractions. The mechanical approach leverages physical force for cervical change, whereas dinoprostone uses targeted receptor-mediated biochemical pathways to facilitate labor initiation.
Efficacy Comparison: Foley Catheter vs. Dinoprostone
The Foley catheter demonstrates comparable efficacy to dinoprostone in cervical ripening and labor induction, with studies reporting similar rates of vaginal delivery within 24 hours. Mechanical methods like the Foley catheter offer a lower risk of uterine hyperstimulation compared to pharmacological agents such as dinoprostone. Both approaches achieve effective cervical dilation, though patient-specific factors and clinical settings often guide the choice between the two.
Safety and Side Effect Profiles
Mechanical methods such as Foley catheters provide a lower risk of systemic side effects compared to Dinoprostone, which is associated with uterine hyperstimulation and fetal heart rate abnormalities. Foley catheters typically cause minimal maternal side effects and are linked to a reduced incidence of tachysystole, making them safer for patients with contraindications to prostaglandins. Dinoprostone's side effect profile includes nausea, vomiting, and fever, whereas mechanical methods primarily carry risks related to infection or discomfort at the insertion site.
Patient Experience and Comfort
Mechanical methods like Foley catheters offer a less pharmacological approach to cervical ripening, often reducing the risk of systemic side effects compared to dinoprostone. Patient comfort can vary; Foley catheters may cause discomfort or cramping during insertion and while in place, whereas dinoprostone administration is typically associated with localized uterine contractions and possible nausea. Studies indicate that patient preference often hinges on the balance between the mechanical sensation and tolerability of medication-related side effects, emphasizing the need for individualized care in labor induction protocols.
Clinical Indications and Contraindications
Mechanical methods like Foley catheters are clinically indicated for cervical ripening in women with a high risk of uterine hyperstimulation or when prostaglandins are contraindicated, such as in cases of previous uterine surgery or asthma. Dinoprostone, a prostaglandin E2 analog, is preferred for labor induction in patients without a history of cesarean delivery or hypersensitivity to prostaglandins. Contraindications for mechanical methods include active genital infections and placenta previa, whereas dinoprostone is contraindicated in patients with non-reassuring fetal status or unexplained vaginal bleeding.
Cost-Effectiveness and Accessibility
Mechanical methods such as Foley catheters provide a cost-effective alternative for labor induction compared to dinoprostone, often reducing overall hospital expenses due to lower medication costs and minimal refrigeration needs. Accessibility is enhanced with Foley catheters as they do not require cold storage, allowing widespread use in low-resource settings where dinoprostone availability may be limited. Studies indicate that while both methods have comparable efficacy, Foley catheters offer significant economic and logistical advantages, improving patient access and reducing healthcare system burdens.
Summary and Recommendations
Mechanical methods such as Foley catheters promote cervical ripening by physically dilating the cervix, offering a low-risk, drug-free alternative for labor induction. Dinoprostone, a prostaglandin E2 analog, chemically softens and dilates the cervix but may carry higher risks of uterine hyperstimulation and fetal distress. Clinical guidelines recommend mechanical methods for patients with contraindications to prostaglandins or higher risk profiles, while Dinoprostone remains effective for standard induction cases, emphasizing individualized choice based on patient safety and efficacy considerations.
Mechanical methods (e.g., Foley catheter) Infographic