Dysplasia refers to the abnormal growth and development of cells, often considered a precancerous condition that may progress to carcinoma if left untreated. Carcinoma is a malignant tumor arising from epithelial cells, representing an invasive and potentially life-threatening form of cancer. Explore the rest of this article to understand how early detection and treatment of dysplasia can impact your health outcomes.
Table of Comparison
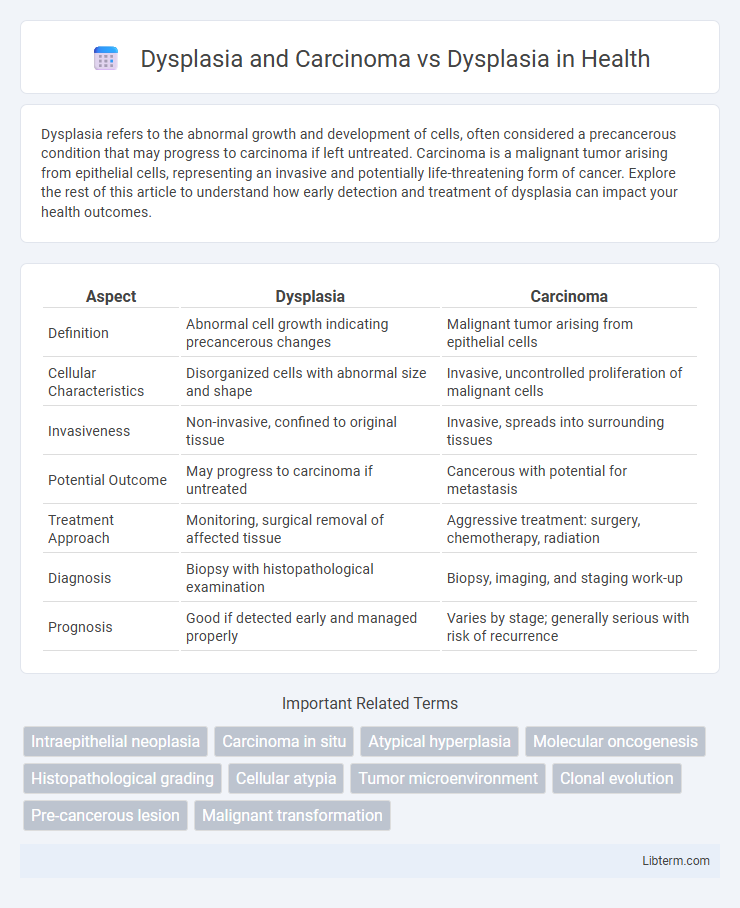
| Aspect | Dysplasia | Carcinoma |
|---|---|---|
| Definition | Abnormal cell growth indicating precancerous changes | Malignant tumor arising from epithelial cells |
| Cellular Characteristics | Disorganized cells with abnormal size and shape | Invasive, uncontrolled proliferation of malignant cells |
| Invasiveness | Non-invasive, confined to original tissue | Invasive, spreads into surrounding tissues |
| Potential Outcome | May progress to carcinoma if untreated | Cancerous with potential for metastasis |
| Treatment Approach | Monitoring, surgical removal of affected tissue | Aggressive treatment: surgery, chemotherapy, radiation |
| Diagnosis | Biopsy with histopathological examination | Biopsy, imaging, and staging work-up |
| Prognosis | Good if detected early and managed properly | Varies by stage; generally serious with risk of recurrence |
Understanding Dysplasia: Definition and Types
Dysplasia refers to the abnormal growth and development of cells within tissues, often considered a pre-cancerous condition with varying degrees classified as mild, moderate, or severe based on cellular disorganization. This cellular atypia can progress to carcinoma, which is an invasive cancer originating from epithelial cells. Understanding the distinct types of dysplasia--such as cervical, oral, or colonic--helps in early diagnosis and intervention to prevent malignant transformation into carcinoma.
What is Carcinoma? Key Characteristics
Carcinoma is a malignant tumor originating from epithelial cells, characterized by uncontrolled cell growth, invasion into surrounding tissues, and potential metastasis. Key features include abnormal cellular morphology, high mitotic activity, and loss of normal tissue architecture, distinguishing it from dysplasia, which involves disorganized but non-invasive epithelial cell growth. Carcinoma often requires aggressive treatment due to its capacity for rapid progression and spread.
Dysplasia vs Carcinoma: Core Differences
Dysplasia refers to the abnormal growth and development of cells within tissues, often considered a precancerous condition, whereas carcinoma represents a malignant tumor arising from epithelial cells with invasive potential. Dysplasia is characterized by cellular atypia and disorganized tissue architecture but lacks the ability to invade beyond the basement membrane, which contrasts with carcinoma's hallmark of local tissue invasion and potential metastasis. Understanding the progression from dysplasia to carcinoma is critical for early diagnosis and intervention in cancer prevention.
Stages of Cellular Transformation: From Dysplasia to Carcinoma
Dysplasia represents an early stage of abnormal cellular transformation characterized by disorganized growth and atypical cell morphology, often considered a precancerous condition. As dysplasia progresses, cellular abnormalities intensify, leading to carcinoma in situ where malignant cells are confined within the epithelial layer without invasion. Transition to invasive carcinoma occurs when these malignant cells breach the basement membrane, enabling metastasis and marking a critical stage in cancer development.
Histopathological Features: Dysplasia and Carcinoma
Dysplasia exhibits cellular atypia with disorganized epithelial architecture, nuclear pleomorphism, and increased mitotic activity without invasion beyond the basement membrane, distinguishing it from carcinoma. Carcinoma demonstrates malignant epithelial cells breaching the basement membrane, invading surrounding stroma, and often forming irregular nests or sheets with marked cellular atypia and frequent mitoses. Histopathological features such as loss of polarity, increased nuclear-cytoplasmic ratio, and abnormal mitoses are prominent in dysplasia but become more pronounced and invasive in carcinoma.
Risk Factors for Progression: When Dysplasia Leads to Carcinoma
Dysplasia, characterized by abnormal cellular growth, carries varying risk factors such as chronic inflammation, genetic mutations, and exposure to carcinogens that increase the likelihood of progression to carcinoma. High-grade dysplasia, persistent cellular atypia, and molecular alterations in genes like TP53 significantly elevate the risk of malignant transformation. Monitoring these risk factors through histopathological evaluation and biomarker analysis is crucial for early intervention and preventing carcinoma development.
Clinical Presentation: Signs and Symptoms
Dysplasia typically presents with asymptomatic cellular abnormalities detected during routine screenings, showing no overt clinical signs, whereas carcinoma often manifests with more pronounced symptoms such as palpable masses, ulcerations, or bleeding depending on the tumor location. Early-stage carcinoma may still lack symptoms, but progressive dysplasia can lead to tissue disorganization and signs like altered mucosal texture or color changes. Clinical vigilance is essential for early identification, especially in high-risk patients, as symptomatic presentation often indicates advanced malignant transformation from dysplasia to carcinoma.
Diagnosis and Screening: Methods and Markers
Diagnosis of dysplasia primarily relies on histopathological examination of biopsy samples, using immunohistochemical markers such as p16 and Ki-67 to distinguish dysplastic changes from benign tissue alterations. Carcinoma diagnosis further incorporates advanced imaging techniques like PET-CT and molecular assays detecting mutations in genes such as TP53 and EGFR for precise tumor characterization. Screening methods include cytology-based tests like Pap smears for cervical dysplasia and biopsy-guided molecular marker analysis, enabling early detection and differentiation between dysplasia and carcinoma.
Management Strategies for Dysplasia and Carcinoma
Management strategies for dysplasia primarily involve close monitoring through regular biopsies and lifestyle modifications to prevent progression, with surgical excision considered for high-grade lesions. Carcinoma requires more aggressive treatment, including surgical resection, radiation therapy, and chemotherapy, tailored to tumor staging and patient health. Early detection and a multidisciplinary approach significantly improve prognosis and survival rates for carcinoma compared to dysplasia.
Prognosis and Survival Outcomes
Dysplasia, characterized by abnormal cell growth, is often considered a precancerous condition with varied potential for progression depending on severity, whereas carcinoma denotes malignant, invasive cancer cells with inherently poorer prognosis. Prognosis and survival outcomes for carcinoma are significantly worse due to tissue invasion and metastasis, contrasting with dysplasia's generally favorable outcome upon early detection and treatment intervention. Clinical management strategies prioritize early dysplasia identification to improve survival rates and prevent progression to carcinoma.
Dysplasia and Carcinoma Infographic