Ezetimibe effectively lowers cholesterol by inhibiting its absorption in the small intestine, making it a key option for managing high LDL levels. It is often prescribed alongside statins to enhance lipid-lowering results, reducing cardiovascular risk. Discover how ezetimibe can improve Your cholesterol management by reading the full article.
Table of Comparison
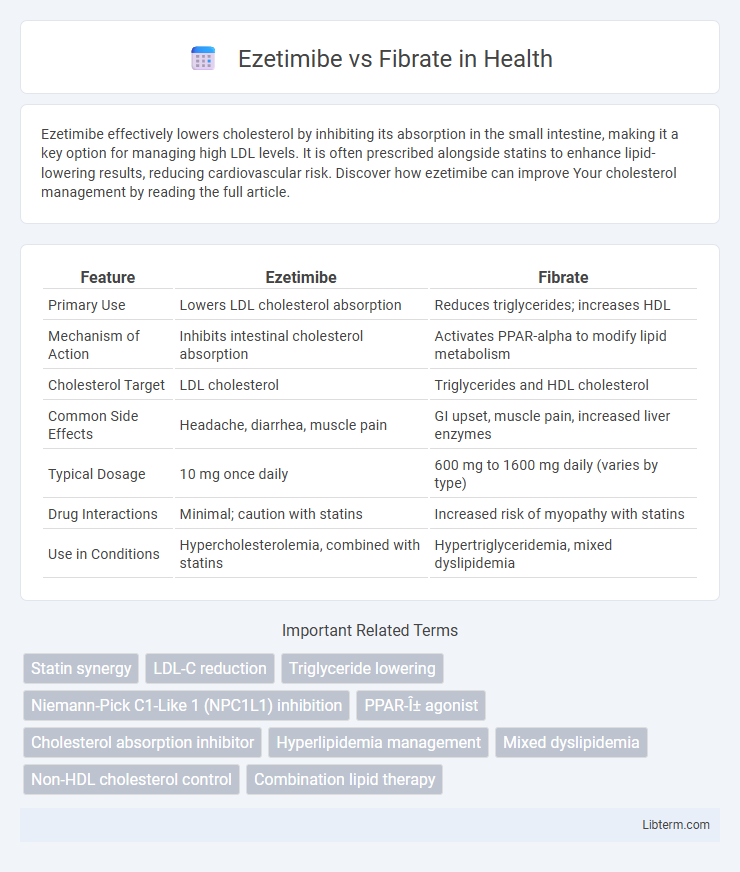
| Feature | Ezetimibe | Fibrate |
|---|---|---|
| Primary Use | Lowers LDL cholesterol absorption | Reduces triglycerides; increases HDL |
| Mechanism of Action | Inhibits intestinal cholesterol absorption | Activates PPAR-alpha to modify lipid metabolism |
| Cholesterol Target | LDL cholesterol | Triglycerides and HDL cholesterol |
| Common Side Effects | Headache, diarrhea, muscle pain | GI upset, muscle pain, increased liver enzymes |
| Typical Dosage | 10 mg once daily | 600 mg to 1600 mg daily (varies by type) |
| Drug Interactions | Minimal; caution with statins | Increased risk of myopathy with statins |
| Use in Conditions | Hypercholesterolemia, combined with statins | Hypertriglyceridemia, mixed dyslipidemia |
Introduction to Ezetimibe and Fibrates
Ezetimibe is a cholesterol absorption inhibitor that targets the Niemann-Pick C1-Like 1 (NPC1L1) protein, effectively reducing low-density lipoprotein cholesterol (LDL-C) levels by preventing dietary cholesterol uptake in the intestines. Fibrates, including gemfibrozil and fenofibrate, are peroxisome proliferator-activated receptor alpha (PPARa) agonists that primarily lower triglycerides and modestly increase high-density lipoprotein cholesterol (HDL-C) by enhancing lipoprotein lipase activity and fatty acid oxidation. Both drug classes play distinct roles in managing dyslipidemia, with ezetimibe mainly focusing on LDL-C reduction and fibrates on triglyceride and HDL-C modulation.
Mechanism of Action: Ezetimibe vs Fibrate
Ezetimibe lowers cholesterol by selectively inhibiting the Niemann-Pick C1-Like 1 (NPC1L1) transporter in the small intestine, reducing the absorption of dietary and biliary cholesterol. Fibrates activate peroxisome proliferator-activated receptors alpha (PPARa), which increase lipoprotein lipase activity and promote the breakdown of triglyceride-rich lipoproteins, enhancing fatty acid oxidation. These distinct mechanisms target different aspects of lipid metabolism to manage dyslipidemia effectively.
Indications and Clinical Uses
Ezetimibe is primarily indicated for the treatment of hypercholesterolemia, effectively reducing low-density lipoprotein cholesterol (LDL-C) by inhibiting intestinal cholesterol absorption. Fibrates, such as gemfibrozil and fenofibrate, are mainly used to manage hypertriglyceridemia and mixed dyslipidemia by activating peroxisome proliferator-activated receptors (PPARs) to enhance lipid metabolism. Clinically, ezetimibe is often prescribed as an adjunct to statins for comprehensive LDL-C control, while fibrates are preferred for patients with elevated triglycerides and low high-density lipoprotein cholesterol (HDL-C).
Efficacy in Lowering Cholesterol Levels
Ezetimibe effectively lowers LDL cholesterol by inhibiting intestinal absorption of cholesterol, resulting in a 15-20% reduction in LDL levels as monotherapy and up to 25-30% when combined with statins. Fibrates primarily target triglycerides and can modestly decrease LDL cholesterol by 5-20%, but their efficacy in lowering LDL is generally inferior to ezetimibe. For patients with high LDL cholesterol, ezetimibe provides superior lipid-lowering effects compared to fibrates, especially in achieving guideline-recommended LDL targets.
Effects on Triglycerides
Ezetimibe primarily lowers LDL cholesterol by inhibiting intestinal cholesterol absorption but has minimal impact on triglyceride levels, typically resulting in modest reductions. Fibrates, such as gemfibrozil and fenofibrate, are more effective at lowering triglycerides, often decreasing levels by 30% to 50% through activation of peroxisome proliferator-activated receptor alpha (PPAR-alpha), which enhances lipolysis and clearance of triglyceride-rich particles. Clinical use favors fibrates for hypertriglyceridemia management, while ezetimibe is preferred for targeting LDL cholesterol with limited triglyceride modification.
Safety Profiles and Side Effects
Ezetimibe primarily lowers LDL cholesterol by inhibiting intestinal absorption and is generally well-tolerated with mild side effects such as headache and gastrointestinal discomfort. Fibrates, which mainly reduce triglycerides and increase HDL cholesterol, carry a higher risk of muscle toxicity, particularly when combined with statins, and may cause gastrointestinal issues and elevated liver enzymes. Both drugs require monitoring for potential adverse effects, but fibrates present a higher incidence of safety concerns compared to the relatively favorable profile of ezetimibe.
Drug Interactions and Contraindications
Ezetimibe primarily interacts with cyclosporine, increasing ezetimibe levels and requiring careful monitoring, while fibrates such as gemfibrozil and fenofibrate intensify the risk of myopathy when combined with statins or other lipid-lowering agents. Contraindications for ezetimibe include active liver disease and unexplained persistent elevations in hepatic transaminases, whereas fibrates are contraindicated in severe renal impairment, hepatic dysfunction, and pre-existing gallbladder disease. Both drug classes necessitate cautious use in patients with chronic kidney disease and close monitoring for muscle-related adverse effects when combined with statins.
Impact on Cardiovascular Outcomes
Ezetimibe significantly reduces low-density lipoprotein cholesterol (LDL-C) by inhibiting intestinal cholesterol absorption, which has been linked to lowered cardiovascular events in large randomized trials like IMPROVE-IT. Fibrates primarily target triglyceride reduction and modestly increase high-density lipoprotein cholesterol (HDL-C), with mixed evidence on their impact on major cardiovascular outcomes, often beneficial in patients with atherogenic dyslipidemia and diabetes. Comparative studies suggest Ezetimibe has a more consistent effect on reducing coronary heart disease risk, especially when added to statin therapy, whereas fibrates may offer benefit in specific metabolic profiles but lack broad cardiovascular event reduction.
Combination Therapy: Ezetimibe and Fibrate
Combination therapy with ezetimibe and fibrates targets distinct lipid pathways, enhancing overall lipid profile management by simultaneously reducing cholesterol absorption and triglyceride synthesis. Clinical studies demonstrate this combination significantly lowers LDL cholesterol and triglycerides more effectively than monotherapy, offering a comprehensive approach for patients with mixed dyslipidemia. Safety profiles indicate tolerability with minimal risk of adverse effects, making ezetimibe-fibrate combinations a valuable option in cardiovascular risk reduction strategies.
Choosing the Right Therapy: Clinical Considerations
Ezetimibe primarily lowers LDL cholesterol by inhibiting intestinal cholesterol absorption, making it suitable for patients with statin intolerance or those needing additional LDL reduction. Fibrates target triglyceride levels and increase HDL cholesterol by activating peroxisome proliferator-activated receptors (PPARs), benefiting patients with hypertriglyceridemia or mixed dyslipidemia. Clinical considerations include the patient's lipid profile, cardiovascular risk, liver and kidney function, and potential drug interactions when selecting between ezetimibe and fibrates for lipid management.
Ezetimibe Infographic