Microcytosis refers to the presence of smaller than normal red blood cells, often indicating underlying conditions like iron deficiency anemia or thalassemia. Identifying the cause of microcytosis is crucial for proper diagnosis and treatment to improve your overall health. Explore the rest of this article to understand the causes, symptoms, and management of microcytosis.
Table of Comparison
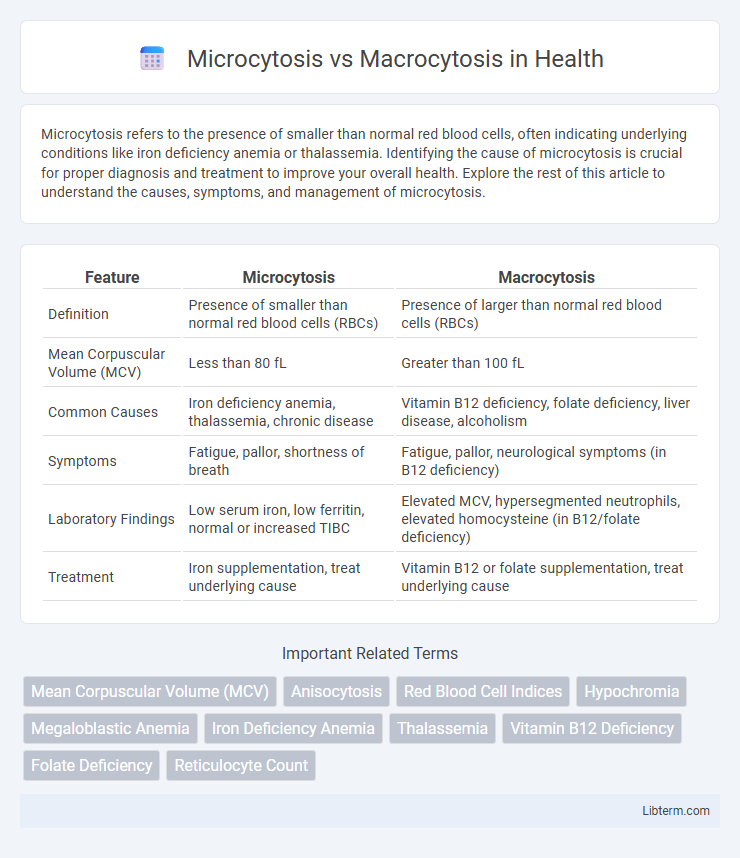
| Feature | Microcytosis | Macrocytosis |
|---|---|---|
| Definition | Presence of smaller than normal red blood cells (RBCs) | Presence of larger than normal red blood cells (RBCs) |
| Mean Corpuscular Volume (MCV) | Less than 80 fL | Greater than 100 fL |
| Common Causes | Iron deficiency anemia, thalassemia, chronic disease | Vitamin B12 deficiency, folate deficiency, liver disease, alcoholism |
| Symptoms | Fatigue, pallor, shortness of breath | Fatigue, pallor, neurological symptoms (in B12 deficiency) |
| Laboratory Findings | Low serum iron, low ferritin, normal or increased TIBC | Elevated MCV, hypersegmented neutrophils, elevated homocysteine (in B12/folate deficiency) |
| Treatment | Iron supplementation, treat underlying cause | Vitamin B12 or folate supplementation, treat underlying cause |
Introduction to Microcytosis and Macrocytosis
Microcytosis is characterized by the presence of abnormally small red blood cells, often associated with iron deficiency anemia or thalassemia, whereas macrocytosis involves enlarged red blood cells commonly linked to vitamin B12 or folate deficiency. Both conditions affect red blood cell size, measured by mean corpuscular volume (MCV), and serve as important diagnostic indicators in hematology. Understanding the underlying causes of microcytosis and macrocytosis aids in targeted treatment and management of various hematologic and systemic disorders.
Defining Microcytosis: Causes and Implications
Microcytosis refers to the presence of smaller-than-normal red blood cells, commonly caused by iron deficiency anemia, thalassemia, and chronic disease inflammation. It results in impaired oxygen delivery and often indicates underlying nutritional deficiencies or genetic disorders. Understanding microcytosis aids in targeted diagnosis and effective management of hematologic conditions distinct from macrocytosis, characterized by enlarged red blood cells.
Understanding Macrocytosis: Key Factors
Macrocytosis is characterized by abnormally large red blood cells with a mean corpuscular volume (MCV) exceeding 100 femtoliters, often caused by vitamin B12 or folate deficiency, liver disease, or bone marrow disorders. The condition can lead to impaired oxygen transport and is frequently detected through complete blood count (CBC) tests. Distinguishing macrocytosis from microcytosis, which features smaller red blood cells and commonly results from iron deficiency or thalassemia, is essential for accurate diagnosis and targeted treatment.
Normal Red Blood Cell Size: Reference Ranges
Normal red blood cell (RBC) size is typically measured by mean corpuscular volume (MCV), with reference ranges of approximately 80-100 femtoliters (fL) in adults. Microcytosis is characterized by an MCV below 80 fL, indicating smaller-than-normal RBCs often seen in iron deficiency anemia and thalassemia. Macrocytosis involves an MCV above 100 fL, reflecting larger RBCs commonly associated with vitamin B12 or folate deficiency and certain bone marrow disorders.
Pathophysiological Differences
Microcytosis is characterized by smaller than normal red blood cells primarily due to impaired hemoglobin synthesis, often associated with iron deficiency or thalassemia, leading to reduced oxygen-carrying capacity. Macrocytosis involves larger red blood cells caused by disrupted DNA synthesis typically stemming from vitamin B12 or folate deficiency, which results in delayed nuclear maturation and cell division. These distinct pathophysiological mechanisms influence red blood cell morphology and underlie differing clinical presentations and diagnostic approaches.
Common Clinical Presentations
Microcytosis typically presents with symptoms of iron deficiency anemia, such as fatigue, pallor, and dyspnea on exertion, often associated with conditions like thalassemia or chronic blood loss. Macrocytosis is commonly observed in vitamin B12 or folate deficiency, with clinical signs including glossitis, neuropathies, and neurological impairments, frequently linked to megaloblastic anemia or liver disease. Both conditions require specific hematologic evaluation using mean corpuscular volume (MCV) to distinguish between small and large red blood cells for accurate diagnosis and treatment.
Diagnostic Approaches and Laboratory Tests
Microcytosis and macrocytosis are hematological conditions characterized by abnormally small and large red blood cells, respectively, with diagnostic approaches relying on complete blood count (CBC) and red cell indices such as mean corpuscular volume (MCV) to differentiate them. Laboratory tests including iron studies (serum iron, ferritin, total iron-binding capacity) and hemoglobin electrophoresis are crucial for diagnosing microcytosis causes like iron deficiency anemia and thalassemias. For macrocytosis, vitamin B12 and folate levels, liver function tests, and bone marrow examination help identify underlying causes such as megaloblastic anemia or liver disease.
Differential Diagnosis: Comparing Both Conditions
Microcytosis, characterized by abnormally small red blood cells, is commonly linked to iron deficiency anemia, thalassemia, and chronic disease-related anemia, whereas macrocytosis involves enlarged red blood cells, often associated with vitamin B12 or folate deficiency, liver disease, and certain myelodysplastic syndromes. Differential diagnosis hinges on blood smear analysis, reticulocyte count, and specific laboratory tests such as serum ferritin, vitamin B12, and folate levels to distinguish underlying causes. Evaluating clinical history alongside hematological parameters ensures accurate identification and appropriate management of these contrasting erythrocyte size disorders.
Treatment Strategies for Microcytosis and Macrocytosis
Treatment strategies for microcytosis primarily focus on addressing the underlying causes such as iron deficiency anemia, often involving oral or intravenous iron supplementation and dietary modifications to increase iron intake. Macrocytosis treatment targets the specific etiologies like vitamin B12 or folate deficiency, managed through vitamin B12 injections or oral folate supplements, with consideration of underlying conditions such as alcoholism or hypothyroidism. Both conditions require tailored diagnostic evaluation to guide appropriate therapy and monitor hematologic response effectively.
Prognosis and Long-Term Outcomes
Microcytosis, often associated with iron deficiency anemia or thalassemia, generally has a favorable prognosis when the underlying cause is effectively treated, resulting in normalized red blood cell indices and improved oxygen delivery. In contrast, macrocytosis, commonly linked to vitamin B12 or folate deficiencies, liver disease, or bone marrow disorders, may indicate more severe or chronic conditions with variable long-term outcomes depending on timely diagnosis and management. Persistent macrocytosis can lead to complications such as neuropathy or hematological malignancies, whereas untreated microcytosis-related disorders might cause chronic fatigue or cardiac strain.
Microcytosis Infographic