Poikilocytosis refers to the presence of abnormally shaped red blood cells in the bloodstream, often indicating underlying health issues such as anemia or bone marrow disorders. Recognizing the types and causes of these irregular cells can help in diagnosing and managing various medical conditions effectively. Discover more about poikilocytosis, its implications, and treatment options by reading the full article.
Table of Comparison
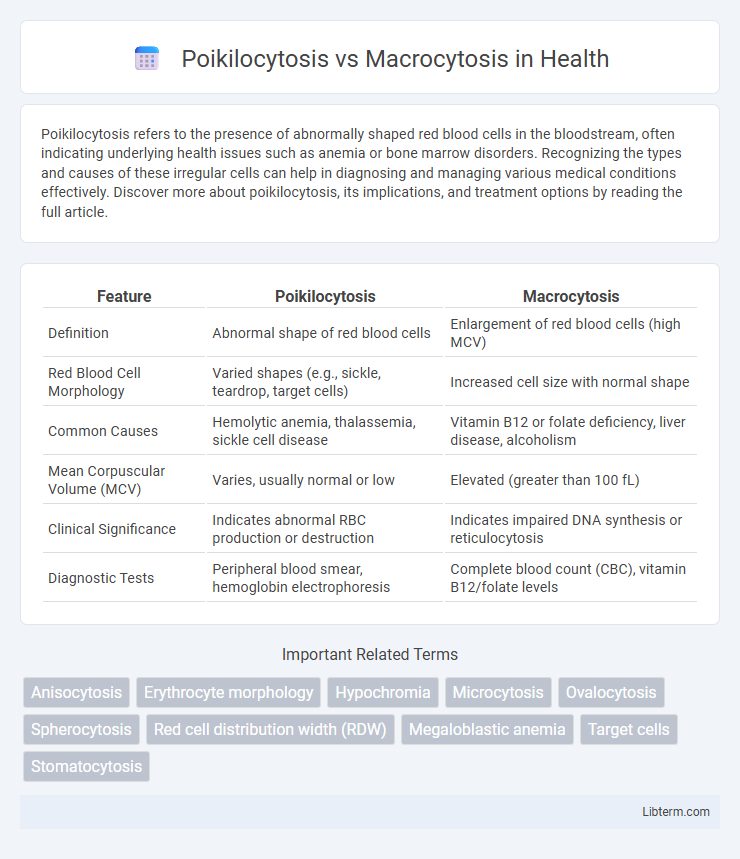
| Feature | Poikilocytosis | Macrocytosis |
|---|---|---|
| Definition | Abnormal shape of red blood cells | Enlargement of red blood cells (high MCV) |
| Red Blood Cell Morphology | Varied shapes (e.g., sickle, teardrop, target cells) | Increased cell size with normal shape |
| Common Causes | Hemolytic anemia, thalassemia, sickle cell disease | Vitamin B12 or folate deficiency, liver disease, alcoholism |
| Mean Corpuscular Volume (MCV) | Varies, usually normal or low | Elevated (greater than 100 fL) |
| Clinical Significance | Indicates abnormal RBC production or destruction | Indicates impaired DNA synthesis or reticulocytosis |
| Diagnostic Tests | Peripheral blood smear, hemoglobin electrophoresis | Complete blood count (CBC), vitamin B12/folate levels |
Introduction to Poikilocytosis and Macrocytosis
Poikilocytosis refers to the presence of abnormally shaped red blood cells in the bloodstream, often indicating underlying conditions like anemia or bone marrow disorders. Macrocytosis is characterized by larger-than-normal red blood cells, commonly associated with vitamin B12 or folate deficiency, liver disease, or myelodysplastic syndromes. Both conditions serve as critical hematological indicators for diagnosing and monitoring various systemic diseases.
Definitions and Key Differences
Poikilocytosis refers to the presence of abnormally shaped red blood cells in the bloodstream, indicating various underlying pathologies such as anemia or bone marrow disorders. Macrocytosis is characterized by enlarged red blood cells with a mean corpuscular volume (MCV) over 100 fL, often associated with vitamin B12 or folate deficiency. The key difference lies in Poikilocytosis focusing on cell shape abnormalities while Macrocytosis emphasizes cell size enlargement.
Causes of Poikilocytosis
Poikilocytosis is characterized by abnormally shaped red blood cells often caused by conditions such as iron deficiency anemia, thalassemia, or sickle cell disease, whereas macrocytosis involves enlarged red blood cells primarily linked to vitamin B12 or folate deficiency. Causes of poikilocytosis include oxidative damage in hereditary elliptocytosis, membrane defects seen in hereditary spherocytosis, and bone marrow disorders like myelodysplastic syndromes. Iron deficiency disrupts hemoglobin synthesis leading to variable cell shapes, which is a hallmark of poikilocytosis.
Causes of Macrocytosis
Macrocytosis primarily results from vitamin B12 or folate deficiency, leading to impaired DNA synthesis and larger-than-normal red blood cells. Other causes include liver disease, hypothyroidism, alcoholism, and certain medications such as chemotherapy agents. Bone marrow disorders like myelodysplastic syndrome and reticulocytosis also contribute to macrocytosis by producing abnormally large red blood cells.
Pathophysiological Mechanisms
Poikilocytosis involves the presence of abnormally shaped red blood cells caused by disruptions in membrane integrity, cytoskeletal abnormalities, or altered erythropoiesis, often linked to conditions like iron deficiency anemia and hemoglobinopathies. Macrocytosis is characterized by enlarged red blood cells resulting from impaired DNA synthesis due to vitamin B12 or folate deficiency, leading to delayed nuclear maturation and continued cytoplasmic growth in erythroid precursors. Both conditions reflect underlying disruptions in red blood cell production and morphology but differ fundamentally in their cellular pathophysiology and associated nutrient deficiencies.
Clinical Manifestations
Poikilocytosis presents clinically with variable-shaped red blood cells leading to symptoms such as fatigue, pallor, and signs of anemia due to impaired oxygen delivery. Macrocytosis is characterized by abnormally large red blood cells causing manifestations like glossitis, neurologic deficits, and megaloblastic anemia related to vitamin B12 or folate deficiency. Both conditions often exhibit overlapping symptoms but require distinct diagnostic evaluation to determine underlying causes and appropriate treatment.
Diagnostic Approaches
Poikilocytosis diagnosis primarily involves peripheral blood smear examination to identify abnormal red blood cell shapes, supplemented by complete blood count (CBC) and reticulocyte count to evaluate anemia severity and bone marrow response. Macrocytosis diagnosis relies on CBC revealing an increased mean corpuscular volume (MCV), with further tests including vitamin B12 and folate levels, liver function tests, and bone marrow biopsy to determine underlying causes such as megaloblastic anemia or liver disease. Both conditions require targeted laboratory investigations to differentiate morphological changes and guide appropriate clinical management.
Laboratory Findings and Blood Smear Features
Poikilocytosis is characterized by a significant variation in red blood cell (RBC) shapes visible on blood smears, including teardrop, oval, or fragmented cells, often detected in conditions such as iron deficiency anemia or myelofibrosis. Macrocytosis presents with increased mean corpuscular volume (MCV >100 fL) and the presence of abnormally large RBCs, often oval macrocytes, seen in vitamin B12 or folate deficiency and liver disease. Laboratory findings in poikilocytosis focus on morphology abnormalities without necessarily elevated MCV, whereas macrocytosis highlights enlarged RBC size with potential hypersegmented neutrophils in smear examination.
Treatment and Management Strategies
Treatment of poikilocytosis involves addressing underlying causes such as nutritional deficiencies or hemolytic anemia, often requiring supplementation with iron, vitamin B12, or folate. Management of macrocytosis typically targets deficiencies in vitamin B12 or folate, with intramuscular vitamin B12 injections or oral folic acid supplements being common interventions. Regular monitoring of blood counts and periodic evaluation of bone marrow function are crucial for both conditions to ensure effective response to therapy and adjust treatment plans accordingly.
Prognosis and Clinical Implications
Poikilocytosis, characterized by abnormally shaped red blood cells, often indicates underlying conditions such as anemia, liver disease, or bone marrow disorders, with prognosis varying based on the root cause and severity. Macrocytosis, identified by enlarged red blood cells typically exceeding 100 fL in mean corpuscular volume (MCV), suggests deficiencies in vitamin B12 or folate, alcohol use, or myelodysplastic syndromes, influencing prognosis through potential neurological complications or marrow failure. Both conditions require targeted diagnostics for effective management; untreated poikilocytosis or macrocytosis can lead to progressive anemia, organ dysfunction, and worsened patient outcomes.
Poikilocytosis Infographic