Megacolon and volvulus are serious gastrointestinal conditions that cause severe bowel enlargement and twisting, leading to obstructed digestion and potential tissue damage. Early recognition and treatment of these disorders are crucial to prevent complications like perforation or ischemia. Discover more about symptoms, causes, and treatment options to protect your digestive health.
Table of Comparison
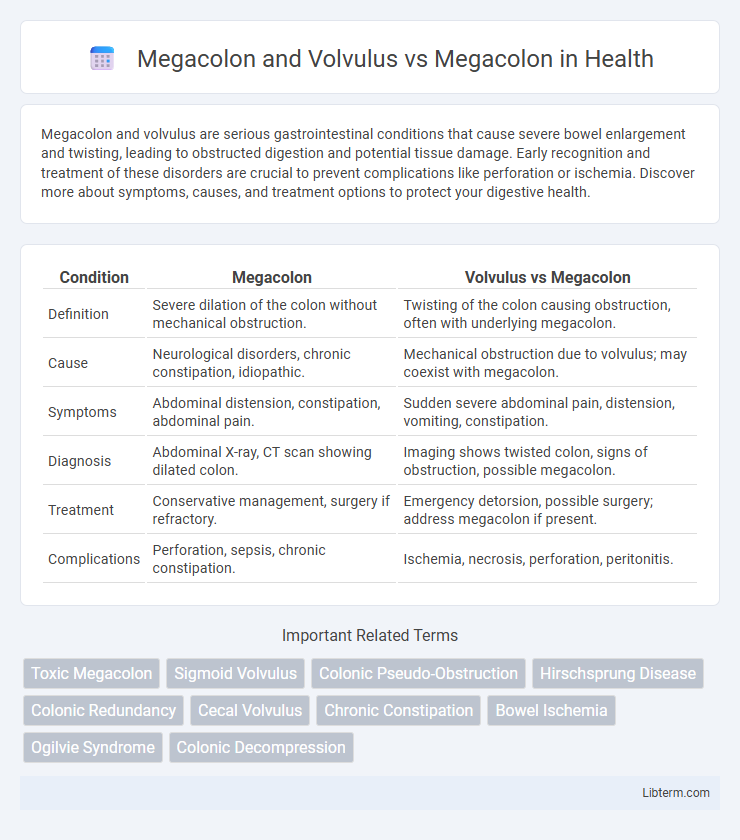
| Condition | Megacolon | Volvulus vs Megacolon |
|---|---|---|
| Definition | Severe dilation of the colon without mechanical obstruction. | Twisting of the colon causing obstruction, often with underlying megacolon. |
| Cause | Neurological disorders, chronic constipation, idiopathic. | Mechanical obstruction due to volvulus; may coexist with megacolon. |
| Symptoms | Abdominal distension, constipation, abdominal pain. | Sudden severe abdominal pain, distension, vomiting, constipation. |
| Diagnosis | Abdominal X-ray, CT scan showing dilated colon. | Imaging shows twisted colon, signs of obstruction, possible megacolon. |
| Treatment | Conservative management, surgery if refractory. | Emergency detorsion, possible surgery; address megacolon if present. |
| Complications | Perforation, sepsis, chronic constipation. | Ischemia, necrosis, perforation, peritonitis. |
Introduction to Megacolon and Volvulus
Megacolon is characterized by abnormal dilation of the colon, often resulting from chronic constipation, nerve damage, or congenital conditions like Hirschsprung's disease. Volvulus, a specific form of megacolon, occurs when the colon twists around itself, causing obstruction and potential ischemia. Understanding the distinction is essential for diagnosis and treatment, as volvulus requires urgent intervention to prevent severe complications.
Defining Megacolon: Causes and Symptoms
Megacolon is characterized by abnormal dilation of the colon, which results from a loss of nerve cells or muscle function, leading to severe constipation and abdominal distension. Causes include congenital conditions like Hirschsprung's disease, infections, inflammatory diseases, and chronic constipation, with symptoms manifesting as chronic bowel obstruction, abdominal pain, and bloating. Volvulus-associated megacolon involves twisting of the colon that causes acute obstruction and ischemia, distinguishing it from non-twisting megacolon, which primarily results from impaired motility and nerve dysfunction.
Understanding Volvulus: Etiology and Presentation
Volvulus, a critical cause of megacolon, occurs when a segment of the colon twists around itself, leading to bowel obstruction and compromised blood flow. Its etiology often involves congenital malformations, chronic constipation, or anatomical anomalies such as malrotation. Clinically, volvulus presents with acute abdominal pain, distension, constipation, and signs of bowel ischemia, distinguishing it from other forms of megacolon that primarily exhibit chronic colonic dilation without acute twisting.
Pathophysiological Differences Between Megacolon and Volvulus
Megacolon involves abnormal dilation of the colon due to impaired motility and chronic constipation, often linked to neuropathic or myopathic disorders affecting colonic smooth muscle or enteric nervous system. In contrast, volvulus results from torsion of the bowel segment, causing mechanical obstruction and vascular compromise, leading to ischemia and rapid onset of symptoms. The pathophysiological distinction lies in megacolon's functional motility failure versus volvulus's acute anatomical twisting and vascular obstruction.
Risk Factors: Overlapping and Distinct
Risk factors for megacolon and volvulus overlap significantly, with chronic constipation, advanced age, and previous abdominal surgeries contributing to both conditions by promoting colonic dilation and torsion. Distinctly, volvulus risk intensifies with anatomical predispositions such as a redundant sigmoid colon and a narrow mesenteric attachment, while megacolon risk factors also include neurological disorders like Hirschsprung's disease and Chagas disease that impair colonic motility. Recognizing these overlapping and unique risk factors is critical for accurate diagnosis and targeted management of each condition.
Diagnostic Approaches: Megacolon vs Volvulus
Megacolon diagnosis relies heavily on abdominal X-rays revealing colonic dilation, while barium enema studies provide detailed visualization of colonic structure and potential obstructions. Volvulus diagnosis requires urgent imaging such as contrast-enhanced CT scans to identify twisting of the bowel and signs of ischemia, with plain abdominal radiographs showing the classic "coffee bean" sign. Colonoscopy serves both diagnostic and therapeutic roles in volvulus by allowing endoscopic detorsion, which is not applicable in primary megacolon cases.
Imaging Findings in Megacolon and Volvulus
Imaging findings in megacolon and volvulus distinctly highlight the pathological differences; megacolon presents as marked colonic dilation with air-fluid levels visible on abdominal X-rays, while volvulus often shows a characteristic "coffee bean" sign due to the twisted bowel segment on plain radiographs or CT scans. Contrast enemas in volvulus reveal a classic "bird's beak" tapering at the site of the twist, aiding differentiation from uncomplicated megacolon, which lacks this obstruction pattern. CT imaging further assists by identifying twisted mesenteric vessels in volvulus, an absent feature in isolated megacolon, guiding prompt surgical intervention decisions.
Treatment Strategies: Distinguishing Management Approaches
Treatment strategies for megacolon and volvulus differ significantly due to their underlying pathophysiology; megacolon often requires conservative management with bowel rest, laxatives, and enemas, while volvulus demands urgent surgical intervention such as detorsion or resection to prevent ischemia. Chronic megacolon may benefit from pharmacologic therapies targeting motility or, in refractory cases, surgical options like colectomy. Differentiating between these conditions using imaging and clinical presentation is critical for optimizing patient outcomes and preventing complications like bowel necrosis in volvulus.
Prognosis and Complication Rates
Megacolon with volvulus presents a more severe prognosis than isolated megacolon due to the risk of bowel ischemia, necrosis, and perforation, which significantly increases mortality rates. Complication rates in megacolon with volvulus are elevated, including acute bowel obstruction, strangulation, and sepsis, compared to the relatively lower risk of chronic constipation and colonic dilation seen in non-volvulus megacolon cases. Early surgical intervention in volvulus-associated megacolon is critical for improving outcomes and reducing life-threatening complications.
Summary: Key Differences and Clinical Considerations
Megacolon is a pathological dilation of the colon that can be congenital or acquired, whereas volvulus involves the twisting of the colon causing obstruction and ischemia, often presenting as an acute surgical emergency. Key differences lie in etiology and clinical presentation: megacolon primarily causes progressive constipation and abdominal distension, while volvulus results in sudden severe pain, bowel obstruction, and risk of necrosis. Clinical considerations emphasize prompt diagnosis of volvulus via imaging to prevent ischemic complications, whereas management of megacolon often includes addressing underlying causes and monitoring for complications like toxic megacolon.
Megacolon and Volvulus Infographic