Bladder stones are hard mineral deposits that form in the bladder due to concentrated urine or underlying urinary tract issues. These stones can cause discomfort, pain, and difficulty urinating, potentially leading to infection or other complications if untreated. Discover more about the symptoms, causes, and effective treatments for bladder stones in the rest of this article.
Table of Comparison
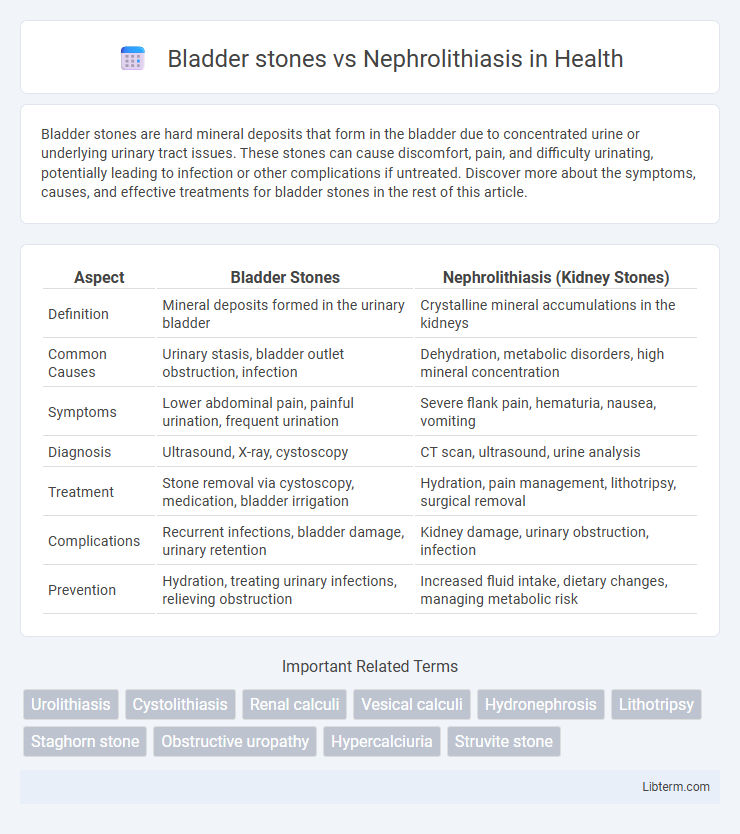
| Aspect | Bladder Stones | Nephrolithiasis (Kidney Stones) |
|---|---|---|
| Definition | Mineral deposits formed in the urinary bladder | Crystalline mineral accumulations in the kidneys |
| Common Causes | Urinary stasis, bladder outlet obstruction, infection | Dehydration, metabolic disorders, high mineral concentration |
| Symptoms | Lower abdominal pain, painful urination, frequent urination | Severe flank pain, hematuria, nausea, vomiting |
| Diagnosis | Ultrasound, X-ray, cystoscopy | CT scan, ultrasound, urine analysis |
| Treatment | Stone removal via cystoscopy, medication, bladder irrigation | Hydration, pain management, lithotripsy, surgical removal |
| Complications | Recurrent infections, bladder damage, urinary retention | Kidney damage, urinary obstruction, infection |
| Prevention | Hydration, treating urinary infections, relieving obstruction | Increased fluid intake, dietary changes, managing metabolic risk |
Introduction to Bladder Stones and Nephrolithiasis
Bladder stones are hardened mineral deposits that form in the bladder, often resulting from urinary stasis or infections. Nephrolithiasis, commonly known as kidney stones, involves the formation of crystalline aggregates within the kidneys due to supersaturation of urinary solutes like calcium, oxalate, or uric acid. Both conditions cause significant urinary tract discomfort and require precise diagnostic imaging such as ultrasound or CT scans for effective management.
Differences in Stone Formation
Bladder stones typically form due to urine retention or bladder outlet obstruction, resulting in concentrated urine that allows mineral crystallization within the bladder. Nephrolithiasis, or kidney stones, primarily originate from supersaturation of urinary solutes like calcium, oxalate, and uric acid in the renal tubules, leading to intrarenal crystal aggregation. Unlike bladder stones that often develop secondary to lower urinary tract issues, nephrolithiasis reflects systemic metabolic imbalances affecting stone nucleation and growth in the kidneys.
Common Causes and Risk Factors
Bladder stones primarily form due to urinary retention caused by bladder outlet obstruction, neurogenic bladder, or chronic infections, while nephrolithiasis originates in the kidneys from supersaturation of urine with minerals like calcium, oxalate, or uric acid. Common risk factors for bladder stones include prostate enlargement, urinary tract infections, and urinary stasis, whereas nephrolithiasis is linked to dehydration, metabolic disorders such as hyperparathyroidism, and dietary factors like high salt or protein intake. Both conditions share overlapping risk factors such as male gender, age over 40, and previous history of urinary stones.
Signs and Symptoms of Each Condition
Bladder stones typically cause lower abdominal pain, frequent urination, painful urination (dysuria), and sometimes hematuria (blood in urine), often accompanied by urinary tract infections. Nephrolithiasis, or kidney stones, often presents with severe flank pain radiating to the groin, hematuria, nausea, vomiting, and sometimes fever if infection is present. Both conditions may lead to urinary obstruction, but the pain location and urinary symptoms help differentiate between bladder stones and nephrolithiasis.
Diagnostic Approaches
Bladder stones are typically diagnosed through imaging techniques such as abdominal X-rays, ultrasound, and cystoscopy, which directly visualize stones within the bladder. Nephrolithiasis diagnosis relies on non-contrast helical CT scans, the gold standard for detecting kidney stones due to their high sensitivity and specificity, alongside urinalysis and blood tests to assess kidney function and stone composition. Both conditions may use intravenous pyelography (IVP) for detailed urinary tract imaging, but CT scans provide superior diagnostic clarity for nephrolithiasis.
Imaging and Laboratory Findings
Bladder stones typically appear as radiopaque densities on plain abdominal X-rays and are confirmed by ultrasound showing echogenic foci with posterior shadowing within the bladder lumen. Nephrolithiasis, or kidney stones, are detected using non-contrast helical CT scans, which provide high sensitivity for stone size, location, and obstruction assessment; laboratory findings often reveal hematuria and variations in serum calcium or uric acid levels depending on stone composition. Urinalysis in bladder stones may show signs of infection or crystals, whereas nephrolithiasis lab tests include 24-hour urine collection for stone risk factors like hypercalciuria or hyperoxaluria.
Treatment Options: Bladder Stones vs. Nephrolithiasis
Treatment options for bladder stones typically involve minimally invasive procedures such as cystolitholapaxy, where stones are broken down and removed via a cystoscope, while larger or complicated stones may require surgical intervention. Nephrolithiasis treatment often includes extracorporeal shock wave lithotripsy (ESWL) to non-invasively fragment kidney stones, alongside medical expulsive therapy using alpha-blockers to facilitate stone passage. Both conditions benefit from hydration and dietary modifications to reduce recurrence, but the choice of treatment depends on stone size, location, and patient health status.
Prevention Strategies and Lifestyle Modifications
Bladder stones prevention focuses on maintaining proper hydration and addressing urinary retention issues to reduce crystal formation in the bladder. Nephrolithiasis prevention involves dietary modifications such as limiting sodium and oxalate intake, increasing citrate-rich foods, and ensuring adequate fluid consumption to decrease kidney stone risk. Regular exercise and managing underlying conditions like hyperparathyroidism and obesity are crucial lifestyle strategies to mitigate both bladder stones and kidney stone development.
Complications and Long-term Outcomes
Bladder stones primarily cause urinary tract infections, bladder irritation, and urinary retention, which can lead to chronic bladder dysfunction and increased risk of bladder cancer if untreated. Nephrolithiasis is associated with complications such as hydronephrosis, renal impairment, and recurrent kidney infections, potentially progressing to chronic kidney disease or renal failure in severe cases. Long-term outcomes for nephrolithiasis depend on stone composition, size, and frequency of recurrence, while bladder stone prognosis improves significantly with timely removal and management of underlying causes.
Summary: Key Differences and Management Considerations
Bladder stones primarily form due to urine stasis or incomplete bladder emptying, while nephrolithiasis involves stone formation within the kidneys, often linked to metabolic abnormalities. Management of bladder stones frequently requires addressing bladder outlet obstruction and removal via cystolitholapaxy, whereas nephrolithiasis treatment emphasizes metabolic evaluation, pain control, hydration, and sometimes extracorporeal shock wave lithotripsy (ESWL) or ureteroscopy. Both conditions necessitate tailored preventive strategies focused on underlying causes to minimize recurrence risks.
Bladder stones Infographic