Sclerotic conditions cause abnormal hardening and loss of flexibility in tissues, impacting organs such as the skin, arteries, and brain. These changes often result in reduced function and can lead to serious health complications if untreated. Discover more about the causes, symptoms, and treatments of sclerotic diseases in the rest of this article.
Table of Comparison
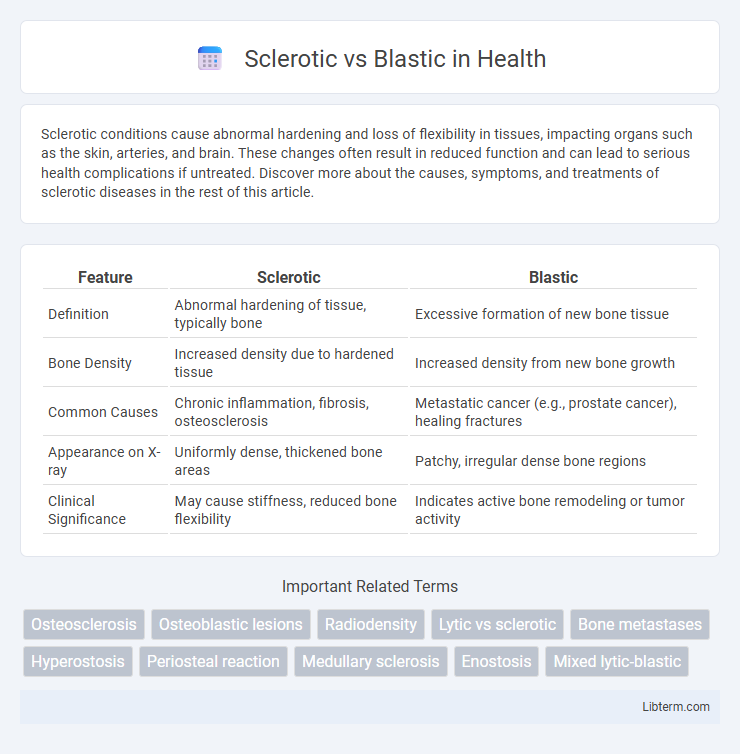
| Feature | Sclerotic | Blastic |
|---|---|---|
| Definition | Abnormal hardening of tissue, typically bone | Excessive formation of new bone tissue |
| Bone Density | Increased density due to hardened tissue | Increased density from new bone growth |
| Common Causes | Chronic inflammation, fibrosis, osteosclerosis | Metastatic cancer (e.g., prostate cancer), healing fractures |
| Appearance on X-ray | Uniformly dense, thickened bone areas | Patchy, irregular dense bone regions |
| Clinical Significance | May cause stiffness, reduced bone flexibility | Indicates active bone remodeling or tumor activity |
Introduction to Sclerotic and Blastic Lesions
Sclerotic lesions are characterized by an abnormal hardening or increased density of bone tissue, commonly observed in metastatic bone disease and conditions like osteoblastic metastases. Blastic lesions represent new bone formation often seen in response to injury or disease, such as in prostate cancer metastases where osteoblastic activity dominates. Understanding the distinction between sclerotic and blastic lesions is critical for accurate diagnosis and treatment planning in oncology and orthopedics.
Defining Sclerotic Lesions
Sclerotic lesions are characterized by increased bone density and hardening, often seen in conditions like osteoblastic metastases or osteosclerosis, indicating abnormal bone formation. In contrast, blastic lesions primarily involve new bone production linked to tumor-induced osteogenesis, frequently observed in prostate cancer metastasis. Distinguishing sclerotic lesions from blastic lesions is essential for accurate diagnosis and targeted treatment planning in bone-related diseases.
Understanding Blastic Lesions
Blastic lesions, also known as osteoblastic lesions, represent areas of increased bone formation characterized by dense, sclerotic bone deposition commonly seen in metastatic bone disease, especially from prostate cancer. These lesions exhibit heightened osteoblast activity leading to abnormal new bone growth, which appears radiographically as dense, hardened regions compared to normal bone tissue. Understanding the nature of blastic lesions is crucial for accurate diagnosis and treatment planning, as they differ from lytic lesions, which involve bone destruction or resorption.
Key Differences: Sclerotic vs Blastic Lesions
Sclerotic lesions are characterized by increased bone density and hardening due to excessive bone formation, commonly seen in conditions like osteoblastic metastases from prostate cancer. Blastic lesions refer specifically to areas of new bone growth produced by osteoblasts, often resulting in irregular, dense bone deposits visible on radiographs. The key difference lies in sclerotic lesions representing a broader category of bone hardening, while blastic lesions specifically denote active new bone formation processes within that sclerotic framework.
Common Causes of Sclerotic Lesions
Sclerotic lesions commonly result from conditions such as metastatic prostate cancer, which frequently produces dense, osteoblastic bone growth, and osteoblastic metastases seen in breast cancer cases. Other causes include Paget's disease, osteopetrosis, and chronic osteomyelitis, all characterized by abnormal hardening or increased bone density. These sclerotic changes contrast with lytic lesions typical of multiple myeloma or renal cell carcinoma, highlighting different pathological processes in bone remodeling.
Common Causes of Blastic Lesions
Blastic lesions are primarily characterized by the abnormal formation of dense, sclerotic bone tissue commonly seen in metastatic prostate cancer, breast cancer, and osteoblastic metastases from lung cancer. These lesions result from increased osteoblastic activity leading to new bone deposition rather than bone resorption, contrasting with sclerotic changes that may involve various benign and malignant conditions. Radiologic evaluation often reveals dense, radiopaque areas on imaging, distinguishing blastic lesions from lytic or mixed lesions caused by different pathologies.
Radiological Features: Comparing Sclerotic and Blastic Patterns
Sclerotic lesions on radiological imaging present as dense, well-defined areas of increased bone density due to new bone formation, commonly seen in conditions like osteoblastic metastases from prostate cancer. Blastic patterns also exhibit increased radiopacity but often show irregular, patchy bone proliferation with less defined margins, reflecting a more aggressive bone response. Differentiating sclerotic from blastic lesions on X-rays, CT, or MRI involves assessing the uniformity, density, and border characteristics to aid in accurate diagnosis and treatment planning.
Clinical Implications and Diagnosis
Sclerotic lesions, characterized by increased bone density, often indicate chronic conditions such as osteoblastic metastases from prostate cancer, while blastic lesions show new bone formation typically linked to osteoblastic activity in diseases like Paget's disease or bone healing. Clinically, differentiating these lesions is crucial as sclerotic changes may signify malignancy requiring biopsy and targeted therapy, whereas blastic patterns suggest active bone remodeling necessitating different diagnostic imaging strategies like bone scintigraphy or MRI. Accurate diagnosis relies on correlating radiographic features with patient history, laboratory markers (e.g., alkaline phosphatase), and tissue biopsy to determine appropriate therapeutic interventions.
Treatment Approaches for Sclerotic and Blastic Lesions
Sclerotic lesions, characterized by increased bone density, often require treatment approaches such as bisphosphonates or radiation therapy to manage pain and prevent fractures. Blastic lesions, involving abnormal bone formation, are typically addressed through systemic therapies like chemotherapy, targeted agents, or radiopharmaceuticals to control tumor growth and bone remodeling. Both lesion types may benefit from multidisciplinary management including orthopedic interventions and supportive care to optimize patient outcomes.
Prognosis and Outcomes
Sclerotic bone lesions typically indicate a slower-growing tumor with a better prognosis, as increased bone density often reflects a reparative or less aggressive process. Blastic lesions, characterized by abnormal new bone formation, are frequently associated with more aggressive malignancies such as prostate cancer metastases, leading to poorer outcomes and increased morbidity. Prognosis in blastic lesions tends to be worse due to rapid disease progression and complications like pathological fractures and spinal cord compression.
Sclerotic Infographic