Restrictive clauses provide essential information that defines or limits the noun they modify, making the meaning of the sentence clearer and more precise. They are crucial in distinguishing specific people, places, or things from a larger group and usually do not require commas. Explore the rest of the article to understand how using restrictive clauses effectively can enhance your writing.
Table of Comparison
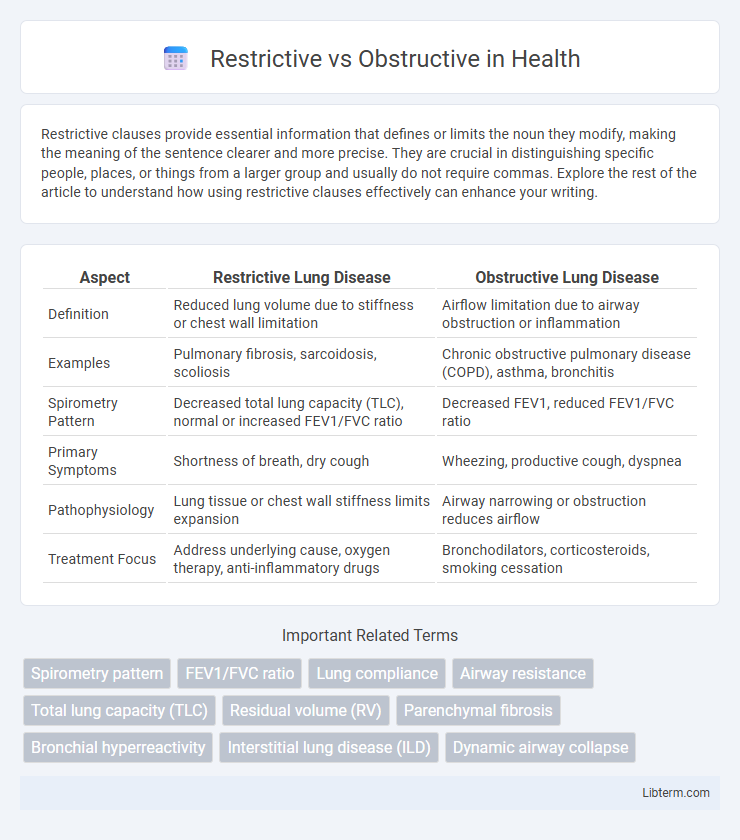
| Aspect | Restrictive Lung Disease | Obstructive Lung Disease |
|---|---|---|
| Definition | Reduced lung volume due to stiffness or chest wall limitation | Airflow limitation due to airway obstruction or inflammation |
| Examples | Pulmonary fibrosis, sarcoidosis, scoliosis | Chronic obstructive pulmonary disease (COPD), asthma, bronchitis |
| Spirometry Pattern | Decreased total lung capacity (TLC), normal or increased FEV1/FVC ratio | Decreased FEV1, reduced FEV1/FVC ratio |
| Primary Symptoms | Shortness of breath, dry cough | Wheezing, productive cough, dyspnea |
| Pathophysiology | Lung tissue or chest wall stiffness limits expansion | Airway narrowing or obstruction reduces airflow |
| Treatment Focus | Address underlying cause, oxygen therapy, anti-inflammatory drugs | Bronchodilators, corticosteroids, smoking cessation |
Overview of Restrictive and Obstructive Disorders
Restrictive and obstructive disorders are two primary categories of respiratory diseases that impair lung function differently. Restrictive disorders, such as pulmonary fibrosis and sarcoidosis, reduce lung expansion and decrease total lung capacity by causing stiffness in lung tissues or chest wall abnormalities. Obstructive disorders, including asthma, chronic obstructive pulmonary disease (COPD), and bronchiectasis, involve airflow limitation due to airway inflammation, narrowing, or obstruction, which increases airway resistance and reduces expiratory flow rates.
Defining Restrictive Lung Diseases
Restrictive lung diseases are characterized by reduced lung volume and impaired lung expansion, leading to decreased total lung capacity (TLC). This category includes conditions such as idiopathic pulmonary fibrosis, sarcoidosis, and pneumoconiosis, where lung tissue stiffness or chest wall abnormalities limit lung inflation. Pulmonary function tests reveal a proportional reduction in forced vital capacity (FVC) and TLC, distinguishing restrictive patterns from obstructive diseases.
Key Characteristics of Obstructive Lung Diseases
Obstructive lung diseases are characterized by airway narrowing and increased resistance, leading to difficulty in exhaling air completely. Key features include reduced forced expiratory volume in one second (FEV1), decreased FEV1/FVC ratio, and air trapping causing lung hyperinflation. Common obstructive diseases include chronic obstructive pulmonary disease (COPD), asthma, bronchiectasis, and cystic fibrosis.
Common Causes of Restrictive Conditions
Restrictive lung diseases commonly arise from conditions such as pulmonary fibrosis, sarcoidosis, and interstitial lung disease, which cause scarring or inflammation that limits lung expansion. Chest wall disorders, including kyphoscoliosis and obesity, also contribute to restrictive patterns by physically restricting lung volume. Neuromuscular diseases like amyotrophic lateral sclerosis (ALS) and muscular dystrophy impair respiratory muscle function, further reducing lung capacity.
Main Causes of Obstructive Conditions
Obstructive conditions in the respiratory system primarily arise from blockages in the airways, with chronic obstructive pulmonary disease (COPD) being the most common cause, often linked to long-term smoking and exposure to environmental pollutants. Other significant causes include asthma, characterized by reversible airway inflammation and bronchoconstriction, and bronchiectasis, which involves permanent airway dilation due to chronic infections and inflammation. These conditions lead to airflow limitation, making it difficult for patients to exhale fully, resulting in symptoms such as wheezing, shortness of breath, and chronic cough.
Differences in Symptoms: Restrictive vs. Obstructive
Restrictive lung diseases cause reduced lung volume, leading to symptoms like shortness of breath during exertion and a rapid, shallow breathing pattern, while obstructive lung diseases feature airflow limitation, causing wheezing, chronic cough, and difficulty exhaling fully. In restrictive conditions, lung compliance is decreased, resulting in stiffness and reduced expansion, whereas obstructive disorders involve airway narrowing or blockage, making air trapping and hyperinflation common. Pulmonary function tests differentiate these by showing a decreased total lung capacity in restrictive diseases versus a reduced forced expiratory volume in one second (FEV1) and an FEV1/FVC ratio below normal in obstructive diseases.
Diagnostic Approaches for Each Disorder Type
Restrictive lung diseases are primarily diagnosed using pulmonary function tests (PFTs) showing reduced total lung capacity (TLC) and preserved airflow (normal or increased FEV1/FVC ratio), supported by imaging techniques like chest X-rays or CT scans revealing interstitial lung fibrosis or chest wall abnormalities. Obstructive lung diseases are diagnosed through spirometry demonstrating decreased FEV1/FVC ratio due to airway narrowing, with further assessments such as bronchodilator responsiveness tests and peak expiratory flow rate measurements to evaluate reversibility. Advanced diagnostic tools including high-resolution CT scans and diffusion capacity tests help differentiate the extent and nature of restrictive versus obstructive pathologies.
Pulmonary Function Test Interpretation
Restrictive lung disease is characterized by reduced lung volumes with a normal or increased FEV1/FVC ratio on pulmonary function tests, indicating difficulty in lung expansion. Obstructive lung disease shows decreased FEV1/FVC ratio due to airflow limitation caused by airway narrowing or obstruction, evident in conditions like asthma and COPD. Key parameters for differentiation include total lung capacity (TLC), which is decreased in restrictive disorders but normal or increased in obstructive diseases.
Treatment Options: Restrictive vs. Obstructive
Treatment options for restrictive lung disease typically involve addressing the underlying cause with anti-inflammatory medications, pulmonary rehabilitation, and supplemental oxygen therapy to improve lung function and reduce symptoms. In contrast, obstructive lung disease treatment focuses on bronchodilators, corticosteroids, and airway clearance techniques to open narrowed airways and manage chronic inflammation. Both conditions may benefit from lifestyle modifications such as smoking cessation and breathing exercises tailored to enhance respiratory efficiency.
Prognosis and Long-Term Management
Restrictive lung diseases typically have a more variable prognosis depending on the underlying cause, with some forms responding well to treatment and others progressing to respiratory failure. Obstructive lung diseases like COPD generally have a chronic, progressive course with long-term management focused on symptom control, smoking cessation, and prevention of exacerbations. Both conditions often require pulmonary rehabilitation, long-term oxygen therapy, and regular monitoring to optimize lung function and improve quality of life.
Restrictive Infographic