Asystole is a critical cardiac emergency characterized by a complete absence of electrical activity in the heart, resulting in no heartbeat and no blood flow. Immediate medical intervention, such as CPR and advanced life support, is essential to increase chances of survival. Discover the key signs, treatment options, and survival tips in the rest of this article.
Table of Comparison
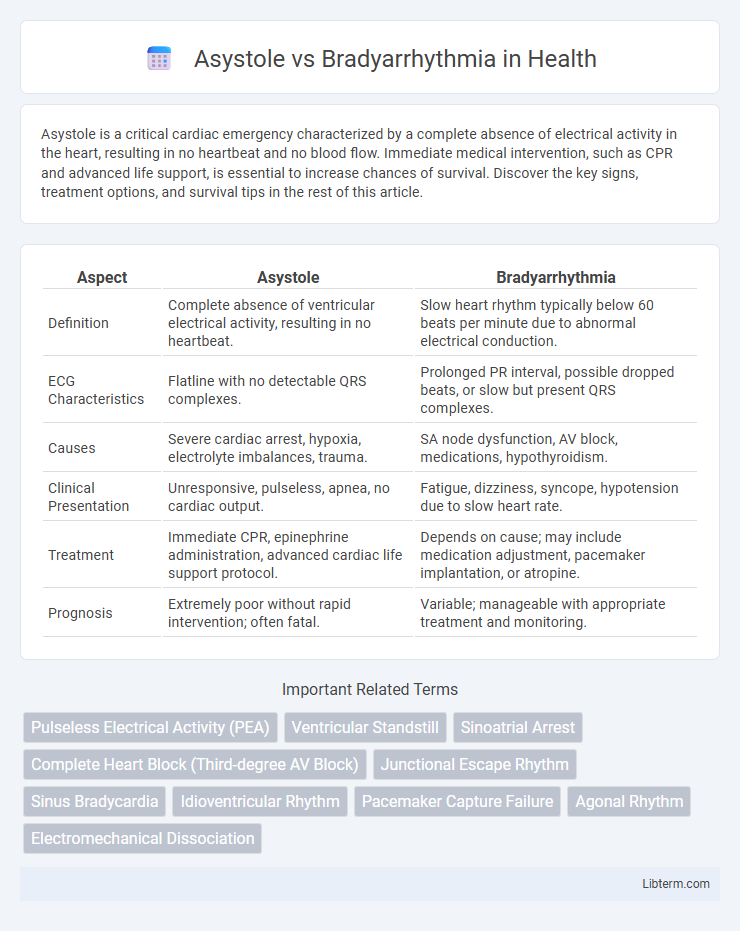
| Aspect | Asystole | Bradyarrhythmia |
|---|---|---|
| Definition | Complete absence of ventricular electrical activity, resulting in no heartbeat. | Slow heart rhythm typically below 60 beats per minute due to abnormal electrical conduction. |
| ECG Characteristics | Flatline with no detectable QRS complexes. | Prolonged PR interval, possible dropped beats, or slow but present QRS complexes. |
| Causes | Severe cardiac arrest, hypoxia, electrolyte imbalances, trauma. | SA node dysfunction, AV block, medications, hypothyroidism. |
| Clinical Presentation | Unresponsive, pulseless, apnea, no cardiac output. | Fatigue, dizziness, syncope, hypotension due to slow heart rate. |
| Treatment | Immediate CPR, epinephrine administration, advanced cardiac life support protocol. | Depends on cause; may include medication adjustment, pacemaker implantation, or atropine. |
| Prognosis | Extremely poor without rapid intervention; often fatal. | Variable; manageable with appropriate treatment and monitoring. |
Introduction to Cardiac Rhythms
Cardiac rhythms encompass a range of electrical activities that regulate heartbeats, where bradyarrhythmia refers to an abnormally slow heart rate usually below 60 beats per minute, often caused by dysfunctions in the sinoatrial node or atrioventricular conduction. Asystole, distinct from bradyarrhythmia, represents a complete absence of electrical activity and ventricular contraction, resulting in a flatline on an electrocardiogram and is considered a cardiac arrest rhythm requiring immediate resuscitation. Understanding the differences between these rhythms is crucial for diagnosing heart conduction abnormalities and guiding appropriate clinical interventions.
What is Asystole?
Asystole is a critical cardiac condition characterized by the complete absence of electrical activity in the heart, resulting in no myocardial contractions and zero cardiac output. ThisZhuang Tai indicates cardiac arrest and requires immediate medical intervention, such as advanced cardiac life support (ACLS) protocols. Unlike bradyarrhythmia, which involves a slow but present heart rhythm, asystole represents a flatline on the electrocardiogram with no detectable heartbeat.
Understanding Bradyarrhythmia
Bradyarrhythmia refers to an abnormally slow heart rhythm, typically defined as a heart rate below 60 beats per minute, caused by dysfunction in the sinoatrial node, atrioventricular node, or His-Purkinje system. This condition can result in inadequate cardiac output, leading to symptoms such as dizziness, fatigue, and syncope. Understanding the underlying causes and electrophysiological mechanisms is essential for distinguishing bradyarrhythmia from asystole, which is a complete absence of electrical activity in the heart.
Key Differences Between Asystole and Bradyarrhythmia
Asystole is characterized by a complete absence of electrical activity in the heart, resulting in no heartbeat, while bradyarrhythmia involves an abnormally slow heart rhythm due to impaired electrical conduction. Asystole presents as a flatline on an electrocardiogram (ECG) and is a form of cardiac arrest requiring immediate resuscitation, whereas bradyarrhythmia shows a slow but present heart rate that may cause symptoms like dizziness or fatigue. Treatment for asystole focuses on advanced cardiac life support (ACLS) protocols, whereas bradyarrhythmia may be managed with medications, pacemaker implantation, or underlying condition correction.
Causes of Asystole
Asystole, characterized by the complete absence of electrical activity in the heart, primarily results from severe hypoxia, prolonged cardiac arrest, or advanced myocardial infarction leading to total heart muscle failure. Electrolyte imbalances, such as hyperkalemia, and drug overdose, including beta-blockers or calcium channel blockers, also contribute to the onset of asystole. Unlike bradyarrhythmia, which involves slow but present heart rhythms caused by sinoatrial node dysfunction or atrioventricular block, asystole represents a more critical and irreversible cessation of cardiac electrical impulses.
Causes of Bradyarrhythmia
Bradyarrhythmia is primarily caused by dysfunction in the sinoatrial node, atrioventricular node, or the conduction pathways, often resulting from ischemic heart disease, aging, or medication effects such as beta-blockers and calcium channel blockers. Electrolyte imbalances, hypothyroidism, and increased vagal tone can also contribute to the development of bradyarrhythmias. In contrast, asystole is typically a result of severe myocardial ischemia, hypoxia, or advanced conduction system failure leading to complete absence of ventricular electrical activity.
Clinical Presentation and Symptoms
Asystole presents with sudden loss of consciousness, absence of pulse, and apnea due to complete cessation of electrical activity in the heart, requiring immediate resuscitation. Bradyarrhythmia manifests with symptoms like fatigue, dizziness, syncope, and shortness of breath resulting from abnormally slow heart rates that impair cardiac output. Both conditions demand prompt identification, but asystole represents a cardiac arrest state, whereas bradyarrhythmia involves persistent slow heart rhythms affecting organ perfusion.
Diagnostic Approaches
Diagnostic approaches for asystole primarily involve immediate electrocardiogram (ECG) monitoring to detect the absence of electrical cardiac activity, often characterized by a flatline appearance. In contrast, bradyarrhythmia diagnosis requires continuous ECG or Holter monitoring to identify abnormally slow heart rhythms, typically below 60 beats per minute, with possible underlying causes including sinoatrial node dysfunction or atrioventricular block. Advanced imaging techniques such as echocardiography and electrophysiological studies may assist in differentiating the precise etiology and guiding treatment strategies for both conditions.
Treatment and Management Strategies
Asystole requires immediate initiation of advanced cardiac life support (ACLS) with high-quality cardiopulmonary resuscitation (CPR) and administration of epinephrine every 3-5 minutes while confirming the absence of a shockable rhythm, as defibrillation is not indicated. Bradyarrhythmia management depends on the underlying cause but often includes atropine administration to increase heart rate, transcutaneous pacing if atropine is ineffective, and consideration of transvenous pacing or permanent pacemaker insertion for persistent symptomatic bradycardia. Electrolyte correction, medication review, and continuous cardiac monitoring are essential in both conditions to optimize patient outcomes and prevent further deterioration.
Prognosis and Outcomes
Asystole, characterized by a complete cessation of cardiac electrical activity, results in a near-zero chance of spontaneous recovery and carries a poor prognosis with high mortality rates despite resuscitation efforts. Bradyarrhythmia, involving abnormally slow heart rhythms, can have variable outcomes depending on the underlying cause, with some cases responding well to interventions such as pacemaker implantation, leading to improved survival and quality of life. Early diagnosis and appropriate management are crucial for bradyarrhythmia prognosis, while asystole outcomes remain dismal due to the lack of effective reversible treatments.
Asystole Infographic