Oxytocin plays a crucial role in social bonding, childbirth, and emotional regulation, influencing behaviors such as trust and empathy. This neuropeptide is often called the "love hormone" due to its impact on forming connections between individuals. Discover how oxytocin affects your brain and relationships by reading the rest of the article.
Table of Comparison
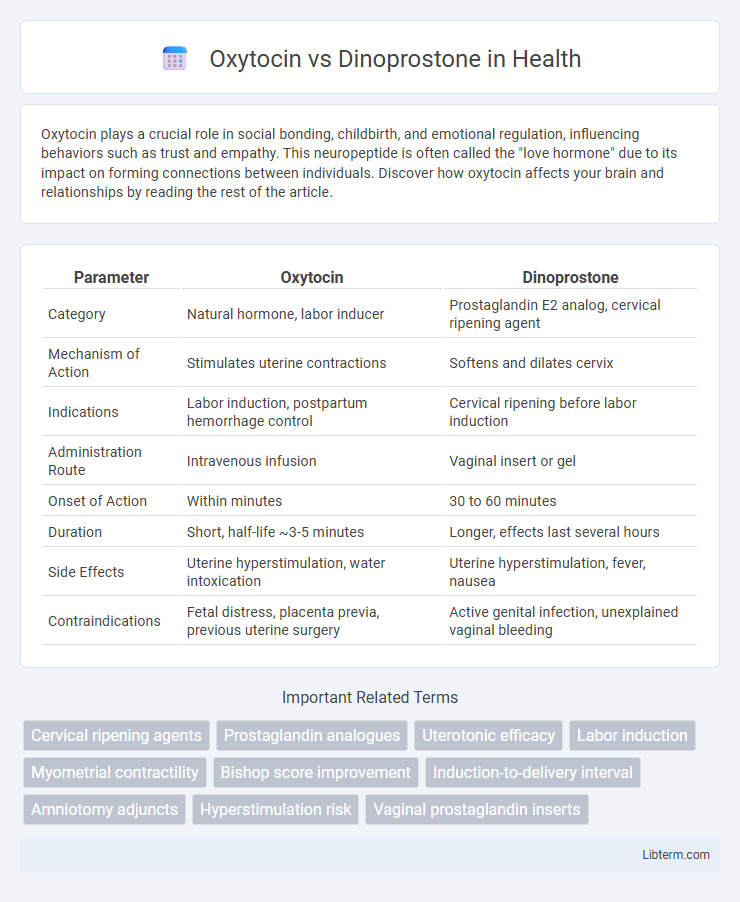
| Parameter | Oxytocin | Dinoprostone |
|---|---|---|
| Category | Natural hormone, labor inducer | Prostaglandin E2 analog, cervical ripening agent |
| Mechanism of Action | Stimulates uterine contractions | Softens and dilates cervix |
| Indications | Labor induction, postpartum hemorrhage control | Cervical ripening before labor induction |
| Administration Route | Intravenous infusion | Vaginal insert or gel |
| Onset of Action | Within minutes | 30 to 60 minutes |
| Duration | Short, half-life ~3-5 minutes | Longer, effects last several hours |
| Side Effects | Uterine hyperstimulation, water intoxication | Uterine hyperstimulation, fever, nausea |
| Contraindications | Fetal distress, placenta previa, previous uterine surgery | Active genital infection, unexplained vaginal bleeding |
Introduction to Oxytocin and Dinoprostone
Oxytocin is a peptide hormone commonly used to induce labor by stimulating uterine contractions, playing a crucial role in childbirth and postpartum hemorrhage management. Dinoprostone, a synthetic prostaglandin E2 analog, is employed to ripen the cervix and initiate labor by promoting cervical softening and uterine contractions. Both agents are integral in obstetrics for labor induction, but they differ in their mechanisms of action and clinical applications.
Mechanism of Action: Oxytocin vs Dinoprostone
Oxytocin acts by binding to oxytocin receptors on uterine smooth muscle, stimulating strong, rhythmic contractions to induce labor. Dinoprostone, a synthetic prostaglandin E2 analogue, binds to prostaglandin receptors, promoting cervical ripening and uterine contraction through increased intracellular calcium. Both agents facilitate labor but differ in receptor targets and pathways, with oxytocin primarily enhancing contractility and dinoprostone modifying cervical tissue and contractile activity.
Indications for Use in Obstetrics
Oxytocin is primarily indicated for induction and augmentation of labor, as well as for controlling postpartum hemorrhage due to uterine atony. Dinoprostone is used for cervical ripening and labor induction in pregnant women at or near term when the cervix is unfavorable. Both agents play crucial roles in obstetric management but target different stages of labor progression.
Administration Methods and Dosages
Oxytocin is typically administered intravenously with a starting dose of 1-2 mU/min, gradually increased by 1-2 mU/min every 30-60 minutes, not exceeding 20 mU/min for labor induction or augmentation. Dinoprostone is delivered either vaginally as a 10 mg insert slowly releasing the drug over 12 hours or as a 20 mcg intracervical gel directly applied for cervical ripening. Precise dosing regimens depend on clinical protocols, with oxytocin requiring continuous monitoring during infusion and dinoprostone allowing for removal of inserts if hyperstimulation occurs.
Efficacy in Labor Induction
Oxytocin demonstrates high efficacy in labor induction by stimulating strong, regular uterine contractions and shortening labor duration compared to Dinoprostone. Dinoprostone, a prostaglandin E2 analog, primarily induces cervical ripening, facilitating labor onset, but may require longer time to active labor and higher risk of uterine hyperstimulation. Clinical studies reveal oxytocin's superior role in progressing active labor phases, while Dinoprostone remains effective in preparing the cervix for induction.
Safety Profiles and Side Effects
Oxytocin and dinoprostone both play crucial roles in labor induction, but their safety profiles differ significantly. Oxytocin, a synthetic hormone, carries risks such as uterine hyperstimulation, fetal distress, and water intoxication, requiring careful dosage monitoring. Dinoprostone, a prostaglandin E2 analog, may cause uterine hypertonus, fever, nausea, and vomiting but is generally preferred for cervical ripening due to a lower incidence of severe fetal complications.
Contraindications and Precautions
Oxytocin is contraindicated in cases of fetal distress, abnormal fetal presentation, and hypersensitivity to the drug, while dinoprostone is contraindicated in patients with a history of uterine surgery or hypersensitivity to prostaglandins. Precautions for oxytocin include monitoring for uterine hyperstimulation and fetal heart rate abnormalities, whereas dinoprostone requires careful observation for uterine rupture, especially in scarred uteri, and possible systemic side effects. Both drugs necessitate cautious use in patients with cardiovascular disorders or asthma due to potential adverse reactions.
Comparative Clinical Studies
Comparative clinical studies reveal that oxytocin is highly effective for inducing labor with a predictable onset and dosage control, while dinoprostone, a prostaglandin E2 analog, offers advantages in cervical ripening and is often preferred in cases with an unripe cervix. Research indicates oxytocin's benefits include shorter labor duration, but dinoprostone may reduce the risk of uterine hyperstimulation and fetal distress. Meta-analyses highlight that combining both agents can optimize labor outcomes by balancing cervix readiness and uterine contractions, improving overall delivery success rates.
Patient Considerations and Preferences
Oxytocin is commonly preferred for labor induction due to its rapid onset and ability to be carefully titrated, but it may cause more intense contractions, which some patients find uncomfortable. Dinoprostone, a prostaglandin E2 analogue, is often chosen for cervical ripening, offering a more gradual onset that can be favorable for patients seeking a less aggressive induction. Patient preferences regarding pain management, previous birth experiences, and concerns about intervention frequency significantly influence the choice between Oxytocin and Dinoprostone.
Summary and Future Perspectives
Oxytocin, a synthetic peptide hormone, is widely used for labor induction due to its strong uterotonic effects, while dinoprostone, a prostaglandin E2 analogue, excels in cervical ripening and preparing the uterus for labor. Emerging studies highlight the potential of combining these agents to enhance efficacy, reduce cesarean rates, and minimize adverse effects during labor. Future research should focus on personalized dosing protocols and novel delivery systems to optimize maternal and neonatal outcomes in diverse clinical settings.
Oxytocin Infographic