Monocytosis indicates an elevated level of monocytes in the bloodstream, often signaling an immune response to infection, inflammation, or certain chronic conditions. Identifying the underlying cause is essential for targeted treatment and monitoring your overall health. Explore the rest of the article to understand the symptoms, causes, and implications of monocytosis.
Table of Comparison
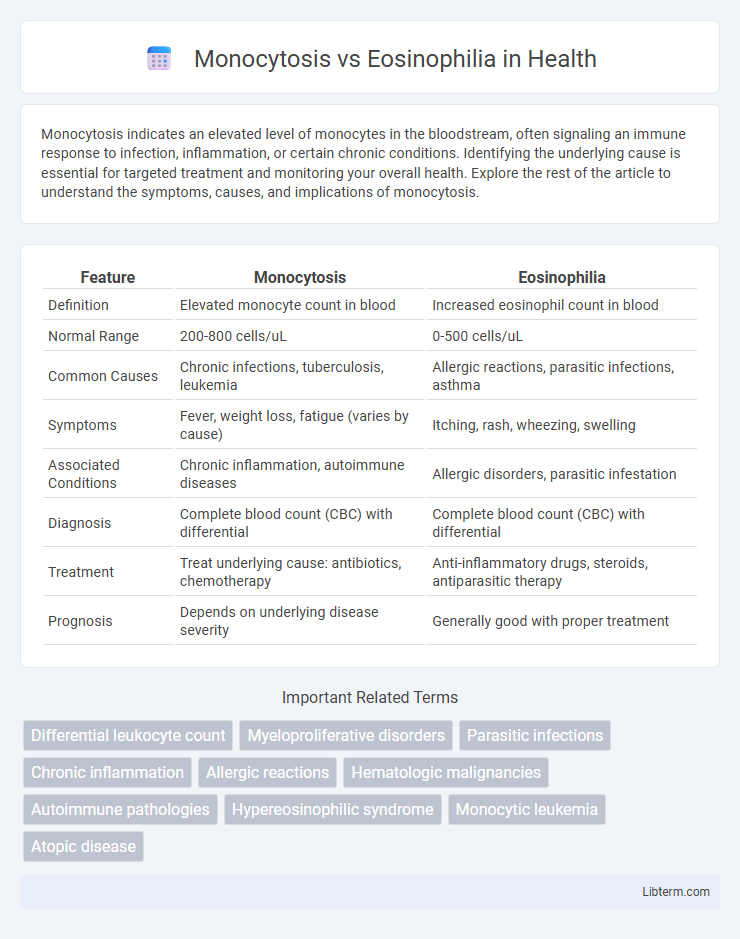
| Feature | Monocytosis | Eosinophilia |
|---|---|---|
| Definition | Elevated monocyte count in blood | Increased eosinophil count in blood |
| Normal Range | 200-800 cells/uL | 0-500 cells/uL |
| Common Causes | Chronic infections, tuberculosis, leukemia | Allergic reactions, parasitic infections, asthma |
| Symptoms | Fever, weight loss, fatigue (varies by cause) | Itching, rash, wheezing, swelling |
| Associated Conditions | Chronic inflammation, autoimmune diseases | Allergic disorders, parasitic infestation |
| Diagnosis | Complete blood count (CBC) with differential | Complete blood count (CBC) with differential |
| Treatment | Treat underlying cause: antibiotics, chemotherapy | Anti-inflammatory drugs, steroids, antiparasitic therapy |
| Prognosis | Depends on underlying disease severity | Generally good with proper treatment |
Understanding Monocytosis and Eosinophilia
Monocytosis is characterized by an elevated monocyte count in the blood, often linked to chronic infections, inflammation, or hematologic disorders, while eosinophilia indicates an increased eosinophil count typically associated with allergic reactions, parasitic infections, or certain cancers. Both conditions reflect immune system responses but differ in cellular focus: monocytes contribute to phagocytosis and antigen presentation, whereas eosinophils primarily target multicellular parasites and modulate allergic inflammation. Accurate diagnosis requires differential blood counts and clinical correlation to identify underlying causes and guide appropriate treatment strategies.
Definitions: Monocytosis vs. Eosinophilia
Monocytosis is defined as an increased number of monocytes in the blood, typically exceeding 800 cells per microliter, often signaling chronic inflammation or infection. Eosinophilia refers to an elevated eosinophil count, usually over 500 cells per microliter, commonly associated with allergic reactions, parasitic infections, or certain autoimmune diseases. These conditions reflect distinct immune responses, with monocytes involved in phagocytosis and tissue repair, while eosinophils primarily target parasites and mediate allergic inflammation.
Causes of Monocytosis
Monocytosis is primarily caused by chronic infections such as tuberculosis, bacterial endocarditis, and viral infections like Epstein-Barr virus, whereas eosinophilia typically results from allergic reactions, parasitic infections, and certain hematologic disorders. Inflammatory conditions including systemic lupus erythematosus and rheumatoid arthritis also contribute to elevated monocyte counts. Monocytosis often reflects ongoing immune response or tissue repair, distinguishing it from eosinophilia's association with hypersensitivity and parasitic defense mechanisms.
Causes of Eosinophilia
Eosinophilia is primarily caused by allergic reactions, parasitic infections, autoimmune diseases, and certain cancers such as Hodgkin lymphoma. Other contributors include drug hypersensitivity, asthma, and eosinophilic gastrointestinal disorders, which lead to elevated eosinophil counts. In contrast, monocytosis results from chronic infections, inflammatory conditions, and hematologic malignancies, distinguishing its etiological profile from eosinophilia.
Clinical Manifestations and Symptoms
Monocytosis manifests with symptoms such as prolonged fever, fatigue, and signs of chronic infections or inflammation, often indicating underlying conditions like tuberculosis or autoimmune diseases. Eosinophilia commonly presents with allergic reactions, asthma, and parasitic infections, showing manifestations like wheezing, skin rashes, and gastrointestinal discomfort. Both conditions require differential diagnosis through blood tests revealing elevated monocyte or eosinophil counts to guide targeted treatment effectively.
Diagnostic Criteria and Laboratory Findings
Monocytosis is diagnosed by an absolute monocyte count exceeding 0.8 x 10^9/L, often linked to chronic infections, inflammation, or hematologic malignancies, with laboratory findings showing elevated monocyte percentages above 8%. Eosinophilia is characterized by an absolute eosinophil count above 0.5 x 10^9/L, commonly associated with allergic reactions, parasitic infections, or certain autoimmune disorders, with peripheral blood smears revealing increased eosinophil granules and elevated serum IgE levels. Differentiating these conditions relies on correlating clinical context with specific leukocyte subtype elevations and additional markers such as C-reactive protein or bone marrow examination in ambiguous cases.
Differential Diagnosis: Key Distinctions
Monocytosis is characterized by an elevated monocyte count often linked to chronic infections, autoimmune disorders, and hematologic malignancies, whereas eosinophilia indicates increased eosinophils typically associated with allergic reactions, parasitic infections, and certain malignancies. Differentiating factors include clinical context, such as symptoms of allergy or parasitosis for eosinophilia, versus signs of chronic inflammation or hematologic disease for monocytosis. Laboratory findings and peripheral blood smear examination play crucial roles in identifying morphological differences and guiding further diagnostic evaluation.
Associated Diseases and Conditions
Monocytosis is commonly associated with chronic infections such as tuberculosis, autoimmune disorders like lupus, and hematologic malignancies including chronic myelomonocytic leukemia. Eosinophilia frequently occurs in allergic diseases, parasitic infections, and certain malignancies such as Hodgkin lymphoma or eosinophilic leukemia. Both conditions reflect different immune response pathways, with monocytosis indicating macrophage activation and eosinophilia signaling hypersensitivity or parasitic response.
Treatment Approaches and Management
Treatment approaches for monocytosis primarily target the underlying causes such as infections, chronic inflammatory diseases, or hematologic disorders, often involving antibiotics, corticosteroids, or chemotherapy depending on etiology. Eosinophilia management focuses on identifying and treating specific triggers like parasitic infections, allergic reactions, or autoimmune diseases, with corticosteroids, antiparasitic agents, or immunomodulatory therapies frequently utilized. Both conditions require ongoing monitoring of blood counts and clinical symptoms to adjust therapy and prevent complications.
Prognosis and Clinical Outcomes
Monocytosis often indicates chronic infections, inflammation, or hematologic disorders with variable prognosis depending on the underlying cause, potentially leading to complications like chronic inflammation or malignancies. Eosinophilia is commonly associated with allergic reactions, parasitic infections, and certain autoimmune diseases, where the clinical outcome hinges on controlling the trigger and preventing organ damage such as eosinophilic myocarditis or pulmonary involvement. Both conditions require targeted treatment to improve prognosis, with persistent elevations warranting further investigation to avoid long-term sequelae.
Monocytosis Infographic