Exenteration is a radical surgical procedure involving the removal of the eye and surrounding structures to treat advanced orbital tumors or severe infections. This complex operation aims to eliminate disease while preserving as much function and appearance as possible. Discover more about the indications, procedure, and recovery of exenteration in the rest of this article.
Table of Comparison
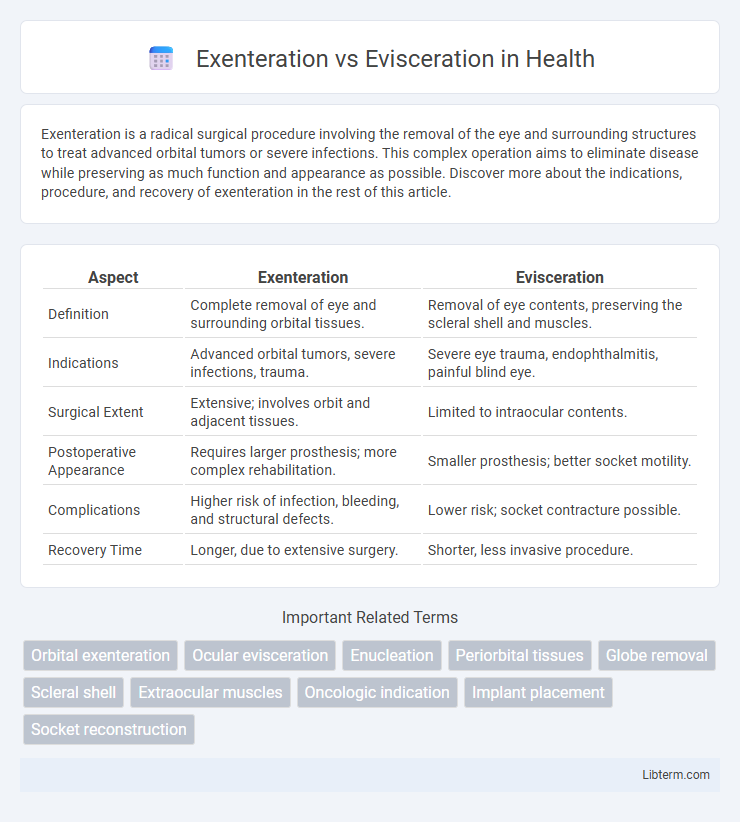
| Aspect | Exenteration | Evisceration |
|---|---|---|
| Definition | Complete removal of eye and surrounding orbital tissues. | Removal of eye contents, preserving the scleral shell and muscles. |
| Indications | Advanced orbital tumors, severe infections, trauma. | Severe eye trauma, endophthalmitis, painful blind eye. |
| Surgical Extent | Extensive; involves orbit and adjacent tissues. | Limited to intraocular contents. |
| Postoperative Appearance | Requires larger prosthesis; more complex rehabilitation. | Smaller prosthesis; better socket motility. |
| Complications | Higher risk of infection, bleeding, and structural defects. | Lower risk; socket contracture possible. |
| Recovery Time | Longer, due to extensive surgery. | Shorter, less invasive procedure. |
Overview of Exenteration and Evisceration
Exenteration involves the complete removal of the eye along with surrounding tissues, including muscles, fat, and sometimes bone, primarily used for extensive orbital tumors or severe infections. Evisceration entails removing the eye's internal contents while preserving the scleral shell and extraocular muscles, typically performed for painful blind eyes or severe ocular trauma. Both procedures aim to alleviate pain or disease but differ significantly in scope and postoperative prosthetic options.
Definitions and Key Distinctions
Exenteration is a radical surgical procedure involving the removal of the entire contents of an orbital cavity, including the eye, surrounding tissues, and sometimes adjacent structures, primarily used to treat aggressive tumors or severe infections. Evisceration refers to the removal of the eye's internal contents while preserving the scleral shell and extraocular muscles, typically performed for endophthalmitis or painful blind eyes. Key distinctions include the extent of tissue removal, with exenteration being more extensive and disfiguring, while evisceration preserves orbital anatomy and often results in better prosthetic outcomes.
Indications for Exenteration
Exenteration is primarily indicated for aggressive malignancies such as orbital sarcomas, recurrent orbital tumors, or invasive squamous cell carcinomas that threaten vital structures. It is reserved for cases where less radical surgeries like evisceration or enucleation fail to achieve tumor control or when the disease involves extensive orbital contents including muscles, fat, and optic nerve. These indications emphasize the need for radical surgical removal to prevent local recurrence and metastasis in advanced orbital cancer.
Indications for Evisceration
Evisceration is primarily indicated for severe ocular trauma, endophthalmitis unresponsive to medical treatment, and painful blind eyes where the sclera remains intact. This procedure involves removing the intraocular contents while preserving the scleral shell, often preferred to maintain orbital anatomy. Evisceration is contraindicated in cases with intraocular malignancy or extensive scleral disease, differentiating it from exenteration that involves complete removal of the eye and surrounding orbital contents.
Surgical Techniques Compared
Exenteration involves the complete removal of the eye along with surrounding structures such as the eyelids, extraocular muscles, and orbital contents, primarily used to treat malignant tumors or severe infections. Evisceration, in contrast, entails removing only the intraocular contents while preserving the scleral shell and extraocular muscles, which allows for better prosthetic motility. Both techniques require precise surgical skill to minimize complications, with exenteration being more radical and evisceration offering faster recovery and improved cosmesis.
Risks and Complications
Exenteration carries risks such as significant blood loss, infection, and potential damage to adjacent structures like the brain or orbit, leading to complex reconstruction challenges. Evisceration poses complications including sympathetic ophthalmia, implant extrusion, and chronic inflammation within the eye socket. Both procedures demand careful postoperative management to mitigate infection and ensure optimal healing outcomes.
Postoperative Recovery and Care
Postoperative recovery after exenteration involves extensive wound care, prolonged hospitalization, and a higher risk of complications like infection and hemorrhage due to the removal of all orbital contents, including eyelids and surrounding tissues. In contrast, evisceration generally entails a shorter recovery period with less intense pain management, as it involves removing intraocular contents while preserving the scleral shell and orbital muscles, allowing quicker prosthesis fitting and better socket motility. Both procedures require diligent follow-up, but exenteration demands more complex rehabilitation, including facial reconstruction and psychological support to address the significant cosmetic and functional deficits.
Functional and Cosmetic Outcomes
Exenteration involves removal of the entire orbital contents including muscles and fat, often leading to significant functional deficits such as loss of ocular movement and vision, requiring complex prosthetic rehabilitation. Evisceration, which removes intraocular contents while preserving the scleral shell and orbital tissues, typically maintains better orbital volume and motility, resulting in improved cosmetic outcomes and easier prosthesis fitting. Functional preservation with evisceration generally facilitates more natural eyelid movement and less socket contracture compared to exenteration, making it preferable when oncologic and infectious indications allow.
Patient Selection Criteria
Exenteration is typically reserved for patients with extensive orbital malignancies or invasive tumors involving multiple orbital structures, where complete removal of the orbital contents is necessary for disease control. Evisceration is suitable for patients with blind, painful eyes due to endophthalmitis or trauma, with intact scleral tissue and no intraorbital malignancy, allowing preservation of the orbital anatomy. Detailed imaging and histopathological evaluation are critical to determine the extent of disease and select the appropriate surgical intervention based on tumor infiltration and ocular integrity.
Long-Term Prognosis and Quality of Life
Exenteration, involving the removal of the entire orbital contents including the eye, typically results in more profound long-term physical and psychological impacts compared to evisceration, which preserves the scleral shell and surrounding tissues. Patients undergoing evisceration often experience better prosthetic mobility and cosmetic outcomes, contributing to improved quality of life and psychosocial adjustment. Long-term prognosis after exenteration may require more complex rehabilitation and carries higher risks of complications, whereas evisceration is associated with fewer postoperative complications and faster functional recovery.
Exenteration Infographic