Somatostatinoma is a rare neuroendocrine tumor that originates in the delta cells of the pancreas or duodenum, leading to excessive secretion of somatostatin. This hormone imbalances digestive processes, causing symptoms such as diabetes, gallstones, and steatorrhea. Discover detailed insights into somatostatinoma symptoms, diagnosis, and treatment options in the rest of this article.
Table of Comparison
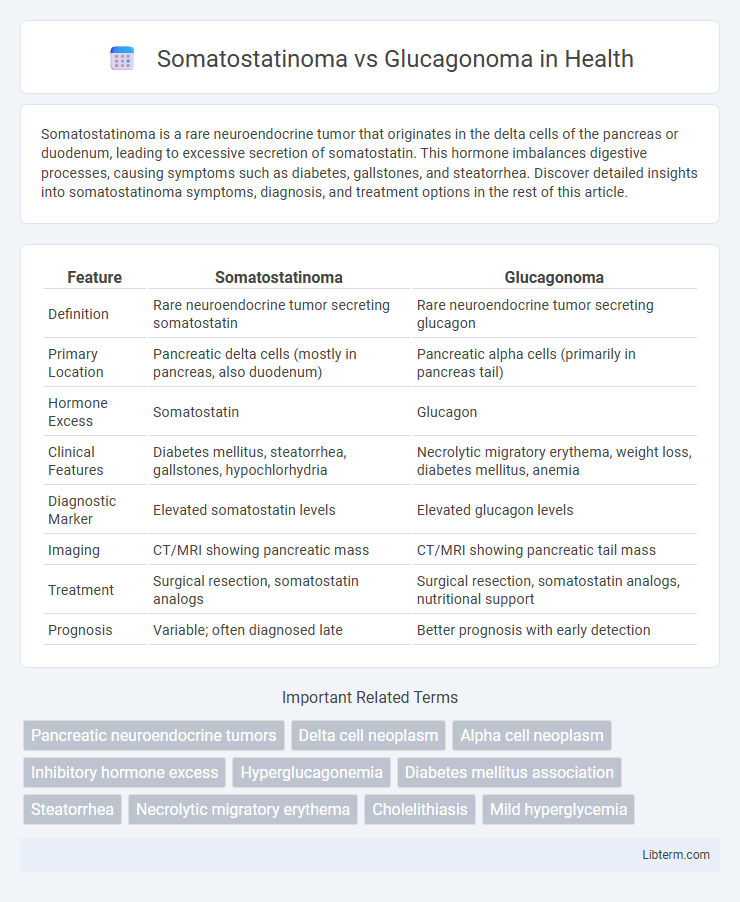
| Feature | Somatostatinoma | Glucagonoma |
|---|---|---|
| Definition | Rare neuroendocrine tumor secreting somatostatin | Rare neuroendocrine tumor secreting glucagon |
| Primary Location | Pancreatic delta cells (mostly in pancreas, also duodenum) | Pancreatic alpha cells (primarily in pancreas tail) |
| Hormone Excess | Somatostatin | Glucagon |
| Clinical Features | Diabetes mellitus, steatorrhea, gallstones, hypochlorhydria | Necrolytic migratory erythema, weight loss, diabetes mellitus, anemia |
| Diagnostic Marker | Elevated somatostatin levels | Elevated glucagon levels |
| Imaging | CT/MRI showing pancreatic mass | CT/MRI showing pancreatic tail mass |
| Treatment | Surgical resection, somatostatin analogs | Surgical resection, somatostatin analogs, nutritional support |
| Prognosis | Variable; often diagnosed late | Better prognosis with early detection |
Overview of Pancreatic Neuroendocrine Tumors
Pancreatic neuroendocrine tumors (PNETs) such as somatostatinomas and glucagonomas arise from the islet cells of the pancreas, each secreting distinct hormones that cause specific clinical syndromes. Somatostatinomas produce excess somatostatin, leading to diabetes, gallstones, and steatorrhea, whereas glucagonomas overproduce glucagon, resulting in hyperglycemia, weight loss, and necrolytic migratory erythema. Both tumors are rare, malignant, and diagnosed using imaging modalities and biochemical assays measuring hormone levels, with treatment involving surgical resection and targeted therapies.
What is Somatostatinoma?
Somatostatinoma is a rare neuroendocrine tumor originating primarily in the pancreas or duodenum that secretes excessive somatostatin, leading to inhibition of several hormones such as insulin and gastrin. This hormonal imbalance causes symptoms including diabetes mellitus, gallbladder stones, and steatorrhea, distinguishing it clinically from glucagonoma which predominantly secretes glucagon and presents with necrolytic migratory erythema. Diagnosis relies on elevated somatostatin levels in plasma and imaging studies like CT or MRI to localize the tumor.
What is Glucagonoma?
Glucagonoma is a rare neuroendocrine tumor originating from the alpha cells of the pancreas, characterized by excessive secretion of the hormone glucagon. This leads to symptoms such as necrolytic migratory erythema, weight loss, diabetes mellitus, and anemia. Unlike somatostatinoma, which secretes somatostatin and causes inhibitory effects on various hormones, glucagonoma primarily causes hyperglycemia due to increased gluconeogenesis and glycogenolysis.
Etiology and Risk Factors
Somatostatinoma primarily arises from delta cells in the pancreas or duodenum and is linked to genetic conditions such as Multiple Endocrine Neoplasia type 1 (MEN1) and Neurofibromatosis type 1 (NF1). Glucagonoma originates from pancreatic alpha cells and is often associated with MEN1 syndrome as well, but unlike somatostatinoma, it can be precipitated by chronic pancreatitis or diabetes mellitus. Both tumors share risk factors related to hereditary syndromes, but their cellular origins and clinical manifestations differ significantly.
Clinical Presentation: Key Differences
Somatostatinomas typically present with diabetes mellitus, steatorrhea, gallstones, and hypochlorhydria due to excessive somatostatin inhibiting various gastrointestinal hormones. In contrast, glucagonomas commonly manifest with diabetes, weight loss, necrolytic migratory erythema, and anemia resulting from elevated glucagon levels affecting glucose metabolism and skin integrity. These distinct clinical features facilitate differentiation between the two rare pancreatic neuroendocrine tumors during diagnosis.
Diagnostic Approaches and Biomarkers
Somatostatinoma diagnosis relies on elevated plasma somatostatin levels and imaging techniques such as MRI and CT to detect pancreatic or duodenal tumors, often accompanied by symptoms like diabetes and cholelithiasis. Glucagonoma is characterized by increased plasma glucagon concentrations, and diagnostic strategies include somatostatin receptor scintigraphy and advanced imaging to localize pancreatic alpha-cell tumors, frequently presenting with necrolytic migratory erythema. Biomarkers such as chromogranin A are elevated in both neuroendocrine tumors, while specific peptide hormone assays provide definitive differentiation between somatostatinoma and glucagonoma.
Imaging and Localization Techniques
Somatostatinomas and glucagonomas are neuroendocrine tumors often localized using advanced imaging techniques such as contrast-enhanced CT and MRI, highlighting hypervascular pancreatic lesions. Somatostatinomas typically appear as well-defined masses in the pancreas or duodenum, with somatostatin receptor scintigraphy and Ga-68 DOTATATE PET/CT improving detection accuracy by targeting somatostatin receptor overexpression. Glucagonomas are localized primarily in the pancreatic tail or body, with functional imaging via PET/CT aiding in identifying metastatic disease and guiding surgical planning through precise tumor mapping.
Management and Treatment Options
Management of somatostatinoma primarily involves surgical resection, with somatostatin analogs such as octreotide used to control hormone-related symptoms and tumor growth. Glucagonoma treatment similarly centers on surgical removal, supported by somatostatin analogs to reduce glucagon secretion and alleviate symptoms like necrolytic migratory erythema and diabetes. Advanced cases of both tumors may require targeted therapies, chemotherapy, or peptide receptor radionuclide therapy (PRRT) for symptom control and tumor shrinkage.
Prognosis and Long-Term Outcomes
Somatostatinomas generally have a poorer prognosis compared to glucagonomas due to their often late diagnosis and aggressive tumor behavior, with 5-year survival rates ranging from 20-40%. In contrast, glucagonomas tend to present earlier with characteristic symptoms like necrolytic migratory erythema, facilitating earlier intervention and leading to better long-term outcomes, with 5-year survival rates around 50-60%. Both neuroendocrine tumors require surgical resection for potential cure, but somatostatinomas have higher risks of metastasis and recurrence, impacting survival negatively.
Comparative Summary: Somatostatinoma vs Glucagonoma
Somatostatinomas are rare neuroendocrine tumors originating from delta cells of the pancreas or duodenum, characterized by excessive somatostatin secretion leading to inhibition of multiple hormonal secretions and symptoms like diabetes, gallstones, and steatorrhea. In contrast, glucagonomas arise from alpha cells of the pancreas and predominantly secrete glucagon, causing hyperglycemia, necrolytic migratory erythema, weight loss, and anemia. Both tumors are diagnosed via elevated hormone-specific plasma levels and imaging studies, with somatostatinomas often linked to diabetes and cholelithiasis, while glucagonomas critically affect glucose metabolism and cutaneous manifestations.
Somatostatinoma Infographic