Hypermagnesemia occurs when magnesium levels in the blood rise above normal, often due to kidney dysfunction or excessive magnesium intake. Symptoms can include nausea, muscle weakness, and irregular heart rhythms, requiring timely diagnosis and treatment to prevent serious complications. Explore the full article to understand the causes, symptoms, and effective management strategies for hypermagnesemia.
Table of Comparison
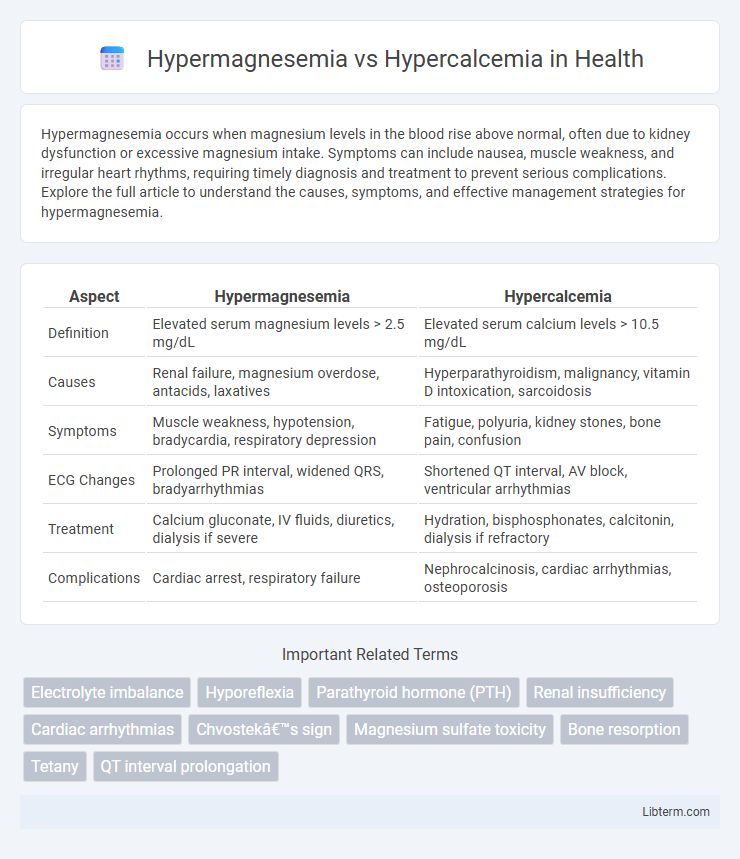
| Aspect | Hypermagnesemia | Hypercalcemia |
|---|---|---|
| Definition | Elevated serum magnesium levels > 2.5 mg/dL | Elevated serum calcium levels > 10.5 mg/dL |
| Causes | Renal failure, magnesium overdose, antacids, laxatives | Hyperparathyroidism, malignancy, vitamin D intoxication, sarcoidosis |
| Symptoms | Muscle weakness, hypotension, bradycardia, respiratory depression | Fatigue, polyuria, kidney stones, bone pain, confusion |
| ECG Changes | Prolonged PR interval, widened QRS, bradyarrhythmias | Shortened QT interval, AV block, ventricular arrhythmias |
| Treatment | Calcium gluconate, IV fluids, diuretics, dialysis if severe | Hydration, bisphosphonates, calcitonin, dialysis if refractory |
| Complications | Cardiac arrest, respiratory failure | Nephrocalcinosis, cardiac arrhythmias, osteoporosis |
Overview of Hypermagnesemia and Hypercalcemia
Hypermagnesemia is characterized by elevated serum magnesium levels, typically above 2.5 mg/dL, often caused by renal failure, excessive magnesium intake, or certain medications. Hypercalcemia involves increased calcium concentration in the blood, usually exceeding 10.5 mg/dL, commonly resulting from hyperparathyroidism, malignancies, or vitamin D intoxication. Both conditions can disrupt neuromuscular and cardiovascular function but differ in etiology, biochemical pathways, and clinical manifestations.
Causes of Hypermagnesemia
Hypermagnesemia primarily results from excessive magnesium intake through supplements or medications, impaired renal function leading to decreased magnesium excretion, and conditions like diabetic ketoacidosis or adrenal insufficiency. Chronic kidney disease is a significant contributing factor as the kidneys fail to adequately filter magnesium, causing its accumulation in the blood. Unlike hypercalcemia, which is often caused by hyperparathyroidism or malignancies, hypermagnesemia is more directly linked to renal impairment and magnesium overload.
Causes of Hypercalcemia
Hypercalcemia is primarily caused by hyperparathyroidism, malignancies such as lung or breast cancer, and excessive vitamin D intake, leading to increased calcium levels in the blood. Other causes include granulomatous diseases like sarcoidosis, certain medications like thiazide diuretics, and prolonged immobilization. In contrast, hypermagnesemia often results from renal failure, magnesium overdose, or excessive use of magnesium-containing antacids or laxatives.
Pathophysiology: How Magnesium and Calcium Affect the Body
Hypermagnesemia results from elevated magnesium levels that depress neuromuscular excitability by blocking calcium channels and reducing acetylcholine release at the neuromuscular junction, leading to muscle weakness and cardiac conduction abnormalities. In contrast, hypercalcemia causes increased calcium deposition in tissues and enhances nerve and muscle excitability initially, but severe cases lead to neuromuscular weakness due to decreased sodium channel permeability. Both electrolyte imbalances disrupt cellular signaling and cardiac rhythm through their effects on ion channel function and membrane potential modulation.
Clinical Manifestations: Symptoms Comparison
Hypermagnesemia commonly presents with symptoms such as muscle weakness, hypotension, nausea, and in severe cases, respiratory depression and cardiac arrhythmias. Hypercalcemia typically manifests with neuropsychiatric symptoms like confusion, fatigue, polyuria, kidney stones, and abdominal pain due to increased gastrointestinal motility. Both conditions can cause cardiac abnormalities, but hypermagnesemia often leads to bradycardia while hypercalcemia may cause shortened QT intervals on ECG.
Laboratory Findings: Diagnostic Differences
Hypermagnesemia typically presents with elevated serum magnesium levels above 2.5 mg/dL, whereas hypercalcemia is defined by serum calcium levels exceeding 10.5 mg/dL. Laboratory findings in hypermagnesemia may also include decreased serum potassium and calcium due to magnesium's inhibitory effect on parathyroid hormone secretion, while hypercalcemia is often accompanied by increased serum phosphorus and elevated parathyroid hormone-related peptide in malignancy cases. Electrolyte panels and magnesium-specific assays aid in differentiating these conditions, with EKG changes such as prolonged PR interval in hypermagnesemia and shortened QT interval in hypercalcemia serving as supportive diagnostic indicators.
Risk Factors and Susceptible Populations
Hypermagnesemia primarily affects patients with chronic kidney disease or those receiving excess magnesium via medications or supplements, as impaired renal function limits magnesium excretion. Hypercalcemia risk factors include malignancies, hyperparathyroidism, and excessive vitamin D intake, commonly impacting older adults and individuals with bone disorders. Both conditions require careful monitoring in hospitalized or critically ill patients due to altered metabolic states and medication effects.
Complications Associated with Each Condition
Hypermagnesemia complications frequently include neuromuscular symptoms such as muscle weakness, hypotonia, and respiratory depression due to impaired calcium influx in nerve cells, while severe cases can lead to cardiac arrhythmias and cardiac arrest. Hypercalcemia primarily causes complications like kidney stones, nephrocalcinosis, and acute kidney injury due to calcium deposition, alongside neuropsychiatric symptoms including confusion, lethargy, and potential coma in extreme cases. Both conditions pose risks of cardiovascular instability, but hypermagnesemia often disrupts conduction through magnesium's effects on ion channels, whereas hypercalcemia alters cardiac contractility and excitability by modulating intracellular calcium levels.
Treatment Strategies for Hypermagnesemia vs Hypercalcemia
Treatment strategies for hypermagnesemia prioritize intravenous calcium gluconate to counteract magnesium's cardiac and neuromuscular effects, alongside aggressive hydration with isotonic saline and loop diuretics to enhance renal magnesium excretion. In contrast, hypercalcemia management involves intravenous fluids for volume expansion, bisphosphonates to inhibit bone resorption, and calcitonin for rapid calcium reduction, especially in malignancy-associated hypercalcemia. Both conditions may require dialysis in severe or refractory cases to promptly normalize electrolyte levels.
Prevention and Long-term Management Approaches
Preventing hypermagnesemia involves careful monitoring of magnesium intake, especially in patients with renal insufficiency, using low-magnesium diets and avoiding magnesium-containing medications. Long-term management focuses on regular assessment of renal function, maintaining balanced electrolyte levels, and patient education on dietary restrictions. In contrast, hypercalcemia prevention requires controlling parathyroid hormone levels and minimizing calcium and vitamin D overconsumption, while long-term strategies include addressing underlying causes such as hyperparathyroidism and ensuring adequate hydration to promote calcium excretion.
Hypermagnesemia Infographic