Intraalveolar procedures involve treatments or interventions conducted within the alveolar bone, crucial for dental and maxillofacial health. Understanding these techniques can enhance your knowledge of advanced dental care and improve patient outcomes by targeting issues inside the alveolar process. Explore the rest of the article to discover detailed insights and practical applications of intraalveolar approaches.
Table of Comparison
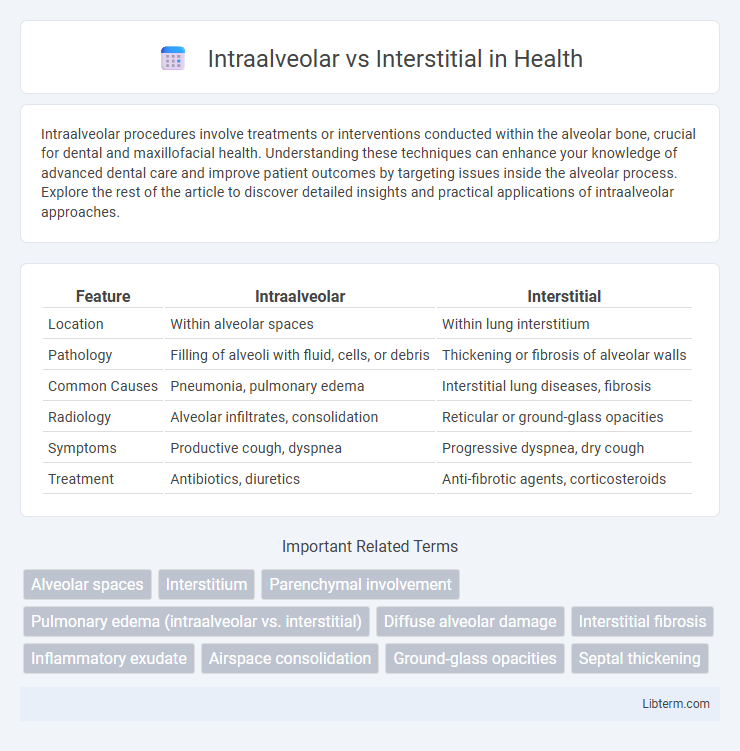
| Feature | Intraalveolar | Interstitial |
|---|---|---|
| Location | Within alveolar spaces | Within lung interstitium |
| Pathology | Filling of alveoli with fluid, cells, or debris | Thickening or fibrosis of alveolar walls |
| Common Causes | Pneumonia, pulmonary edema | Interstitial lung diseases, fibrosis |
| Radiology | Alveolar infiltrates, consolidation | Reticular or ground-glass opacities |
| Symptoms | Productive cough, dyspnea | Progressive dyspnea, dry cough |
| Treatment | Antibiotics, diuretics | Anti-fibrotic agents, corticosteroids |
Understanding Intraalveolar and Interstitial Spaces
Intraalveolar spaces refer to the air-filled cavities within the alveoli where gas exchange occurs, while interstitial spaces encompass the connective tissue and capillaries between alveoli that provide structural support and facilitate fluid balance. The intraalveolar space is critical for oxygen and carbon dioxide diffusion, whereas the interstitial space contains extracellular matrix components like collagen and elastin, influencing lung compliance and elasticity. Understanding the distinction between these spaces is essential for diagnosing and managing pulmonary conditions such as pulmonary edema, where fluid accumulation in the interstitial or intraalveolar spaces alters respiratory function.
Anatomical Differences: Intraalveolar vs Interstitial
Intraalveolar and interstitial spaces differ anatomically by their location relative to the alveoli; intraalveolar spaces are within the alveolar sacs where gas exchange occurs, while the interstitial spaces lie in the tissue surrounding alveoli, including the alveolar walls, capillaries, and connective tissue. The intraalveolar region consists mainly of air-filled cavities that facilitate oxygen and carbon dioxide diffusion, whereas the interstitial area contains structural components such as fibroblasts, collagen, and elastin fibers that maintain lung architecture and support alveolar function. These differences influence pathological processes, with intraalveolar abnormalities primarily affecting airspace filling and interstitial changes impacting lung stiffness and diffusion properties.
Pathophysiology: How Diseases Affect Each Space
Intraalveolar diseases primarily disrupt the alveolar spaces by filling them with fluid, cells, or exudates, impairing gas exchange and leading to conditions such as pulmonary edema or pneumonia. Interstitial diseases target the lung interstitium, causing thickening, fibrosis, or inflammation of the alveolar walls and supporting structures, commonly seen in idiopathic pulmonary fibrosis and interstitial lung diseases (ILDs). These distinct pathophysiological mechanisms affect lung compliance, diffusion capacity, and respiratory function in characteristic ways, guiding diagnosis and treatment strategies.
Common Conditions Involving Intraalveolar Space
Common conditions involving the intraalveolar space include pulmonary edema, pneumonia, and alveolar hemorrhage, where fluid, pus, or blood accumulates within the alveoli, impairing gas exchange. In contrast, interstitial lung diseases like idiopathic pulmonary fibrosis primarily affect the interstitium--the connective tissue surrounding alveoli--leading to thickening and reduced lung compliance. Distinguishing between intraalveolar and interstitial involvement is crucial for accurate diagnosis and targeted treatment in pulmonary medicine.
Common Conditions Involving Interstitial Space
Interstitial space abnormalities commonly occur in conditions such as pulmonary fibrosis, sarcoidosis, and interstitial pneumonia, which lead to thickening and inflammation of the lung interstitium. In contrast, intraalveolar processes mainly involve alveolar spaces and include conditions like pulmonary edema and alveolar hemorrhage, characterized by fluid or cells filling the alveoli. Understanding the distinction between interstitial and intraalveolar involvement is crucial for accurate diagnosis, prognosis, and treatment in respiratory medicine.
Clinical Signs: Intraalveolar vs Interstitial Disorders
Intraalveolar disorders typically present with acute respiratory symptoms such as coughing, frothy sputum, and hypoxemia due to alveolar flooding or hemorrhage, often visible as consolidation on chest X-rays. Interstitial disorders manifest with chronic symptoms including progressive dyspnea, dry cough, and inspiratory crackles, reflecting fibrosis or inflammation of the lung interstitium, which appears as reticular or ground-glass opacities on imaging. Clinical signs like digital clubbing and restrictive lung function patterns are more common in interstitial lung diseases, whereas signs of infection or acute inflammation dominate intraalveolar conditions.
Radiological Features: Distinguishing Alveolar and Interstitial Patterns
Intraalveolar patterns on radiological imaging typically present as airspace opacities with a fluffy, cloud-like appearance, often demonstrating air bronchograms due to alveolar filling. Interstitial patterns show a reticular or nodular texture resulting from thickening of alveolar walls, septa, or the interstitium, and lack air bronchograms. Recognition of these features on chest X-rays or CT scans is crucial for differentiating conditions such as pulmonary edema, pneumonia (intraalveolar), and pulmonary fibrosis or interstitial lung disease (interstitial).
Diagnostic Techniques for Intraalveolar and Interstitial Diseases
Diagnostic techniques for intraalveolar diseases primarily include high-resolution computed tomography (HRCT) to detect alveolar filling patterns and bronchoalveolar lavage (BAL) to analyze cellular components within the alveoli. Interstitial diseases are best diagnosed using HRCT for identifying interstitial thickening, fibrosis, and ground-glass opacities, combined with lung biopsy techniques such as video-assisted thoracoscopic surgery (VATS) to obtain histopathological confirmation. Pulmonary function tests (PFTs) further assist in differentiating the restrictive impairments prevalent in interstitial lung diseases from the alveolar consolidation seen in intraalveolar conditions.
Treatment Approaches: Tailoring to Each Space
Treatment approaches for intraalveolar and interstitial lung diseases differ significantly based on the affected space's pathology. Intraalveolar conditions, such as pulmonary edema or alveolar hemorrhage, often require interventions targeting fluid removal and inflammation reduction, using diuretics, corticosteroids, or immunosuppressants. Interstitial lung diseases demand antifibrotic agents, immunomodulators, and oxygen therapy tailored to halt fibrosis progression and improve lung compliance.
Prognosis and Outcomes: Intraalveolar vs Interstitial Involvement
Intraalveolar involvement typically leads to faster resolution with appropriate treatment due to localized alveolar damage, often seen in conditions like pneumonia. Interstitial involvement generally indicates a more chronic or progressive pathology, such as interstitial lung disease, resulting in poorer prognosis with potential for fibrosis and long-term respiratory impairment. Outcomes for interstitial involvement are often less favorable, requiring vigilant monitoring and advanced therapeutic strategies to manage irreversible lung damage.
Intraalveolar Infographic