Manual vacuum aspiration is a safe and effective procedure used primarily for early pregnancy termination and miscarriage management. It involves the gentle removal of uterine contents using a handheld suction device, minimizing discomfort and recovery time. Discover more about how this method can be performed and what to expect in the rest of the article.
Table of Comparison
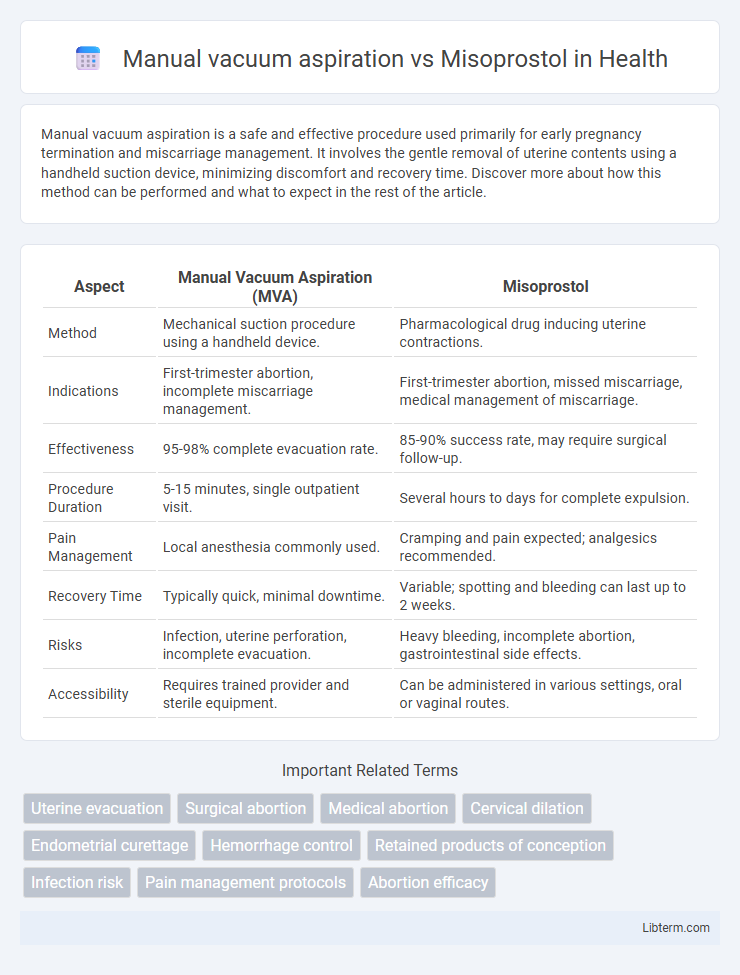
| Aspect | Manual Vacuum Aspiration (MVA) | Misoprostol |
|---|---|---|
| Method | Mechanical suction procedure using a handheld device. | Pharmacological drug inducing uterine contractions. |
| Indications | First-trimester abortion, incomplete miscarriage management. | First-trimester abortion, missed miscarriage, medical management of miscarriage. |
| Effectiveness | 95-98% complete evacuation rate. | 85-90% success rate, may require surgical follow-up. |
| Procedure Duration | 5-15 minutes, single outpatient visit. | Several hours to days for complete expulsion. |
| Pain Management | Local anesthesia commonly used. | Cramping and pain expected; analgesics recommended. |
| Recovery Time | Typically quick, minimal downtime. | Variable; spotting and bleeding can last up to 2 weeks. |
| Risks | Infection, uterine perforation, incomplete evacuation. | Heavy bleeding, incomplete abortion, gastrointestinal side effects. |
| Accessibility | Requires trained provider and sterile equipment. | Can be administered in various settings, oral or vaginal routes. |
Introduction to Manual Vacuum Aspiration and Misoprostol
Manual vacuum aspiration (MVA) is a minimally invasive surgical procedure used for early pregnancy termination or uterine evacuation, involving the use of a hand-held suction device to safely remove uterine contents. Misoprostol is a prostaglandin E1 analog that induces uterine contractions and cervical ripening, making it an effective pharmacological method for medical abortion and management of miscarriage. Both MVA and misoprostol offer safe, effective options for pregnancy termination, with choices influenced by clinical context, patient preference, and resource availability.
Overview of Manual Vacuum Aspiration (MVA)
Manual Vacuum Aspiration (MVA) is a safe and effective outpatient procedure used to evacuate the uterus during early pregnancy termination or miscarriage management, typically up to 12 weeks gestation. It involves the use of a hand-held syringe to create suction, which removes uterine contents with minimal discomfort and reduced risk of infection compared to sharp curettage. MVA offers faster completion, immediate results, and lower complication rates, making it a preferred method in many clinical settings over medical alternatives like Misoprostol.
Overview of Misoprostol for Abortion
Misoprostol is a prostaglandin E1 analogue widely used for medical abortion due to its effectiveness in inducing uterine contractions and cervical dilation. It offers a non-invasive alternative to manual vacuum aspiration by facilitating the expulsion of pregnancy tissue, often administered orally or vaginally. Misoprostol's accessibility, ease of use, and ability to be self-administered make it a valuable option in reproductive healthcare, especially in settings with limited surgical resources.
Mechanism of Action: MVA vs Misoprostol
Manual vacuum aspiration (MVA) operates through mechanical suction to evacuate uterine contents by creating negative pressure in the uterine cavity, effectively removing tissue. Misoprostol induces uterine contractions and cervical ripening by acting as a prostaglandin E1 analog, binding to prostaglandin receptors in the uterus to stimulate smooth muscle activity. The distinct mechanisms--MVA's physical extraction versus Misoprostol's pharmacological induction of contractions--dictate their protocols and clinical applications in uterine evacuation.
Effectiveness and Success Rates
Manual vacuum aspiration (MVA) demonstrates higher immediate success rates, generally around 95-98%, in complete uterine evacuation compared to misoprostol, which shows success rates ranging from 80-90% depending on dosage and gestational age. MVA provides rapid and definitive removal of retained products, reducing the need for follow-up procedures, while misoprostol relies on induced uterine contractions and may require additional doses or surgical intervention if incomplete. Clinical studies indicate MVA as more effective for first-trimester miscarriage management, with faster resolution and lower overall failure rates compared to medical management with misoprostol alone.
Safety and Side Effects Comparison
Manual vacuum aspiration (MVA) offers a high safety profile with a low incidence of complications such as infection and uterine perforation, making it a reliable surgical method for early pregnancy termination. Misoprostol, a pharmacological alternative, commonly causes side effects including cramping, bleeding, nausea, and diarrhea, but serious adverse events are rare when used appropriately. Both methods are considered safe under clinical supervision, with MVA providing immediate completion and Misoprostol allowing non-invasive management, though the latter may require follow-up to confirm efficacy and manage prolonged bleeding.
Pain Management and Comfort Levels
Manual vacuum aspiration (MVA) generally provides more immediate pain relief through local anesthesia and sedation, resulting in lower pain scores during the procedure compared to Misoprostol. Misoprostol, administered orally or vaginally, can cause cramping and discomfort over several hours but avoids invasive instrumentation, which may increase patient comfort post-treatment. Studies indicate MVA is preferred for rapid pain control, while Misoprostol offers a non-surgical option with manageable pain and greater overall comfort in outpatient settings.
Accessibility and Resource Requirements
Manual vacuum aspiration requires specialized equipment and trained personnel, limiting its accessibility in low-resource or remote settings. Misoprostol, being a medication that can be administered orally or sublingually, offers greater accessibility, especially in areas lacking surgical facilities or qualified healthcare providers. The resource-light nature of misoprostol enables broader implementation for uterine evacuation in diverse healthcare environments.
Patient Preferences and Psychological Impact
Patient preferences in managing early pregnancy loss often favor manual vacuum aspiration for its shorter procedure time and immediate completion, providing a sense of control and closure. Misoprostol, as a non-surgical option, appeals to patients prioritizing privacy and avoidance of anesthesia, although it may involve unpredictable bleeding and longer duration, impacting emotional well-being. Psychological outcomes tend to improve with personalized counseling, ensuring that patient values and expectations align with the chosen method to reduce anxiety and enhance satisfaction.
Choosing the Right Method: Key Considerations
When choosing between manual vacuum aspiration (MVA) and misoprostol for early pregnancy termination, factors such as gestational age, medical history, and access to medical facilities play critical roles. MVA offers immediate completion with a high success rate, making it suitable for early pregnancies up to 12 weeks, while misoprostol provides a non-invasive, medication-based option preferred when surgical procedures are less accessible. Patient preference, potential side effects, and the need for follow-up care are essential considerations to ensure safe and effective treatment outcomes.
Manual vacuum aspiration Infographic