Clubfoot is a congenital deformity characterized by the inward twisting of the foot, affecting mobility and daily activities. Early diagnosis and treatment, such as casting, bracing, or surgery, are essential to ensure optimal correction and prevent long-term complications. Discover effective strategies and expert advice to manage your child's clubfoot throughout this comprehensive article.
Table of Comparison
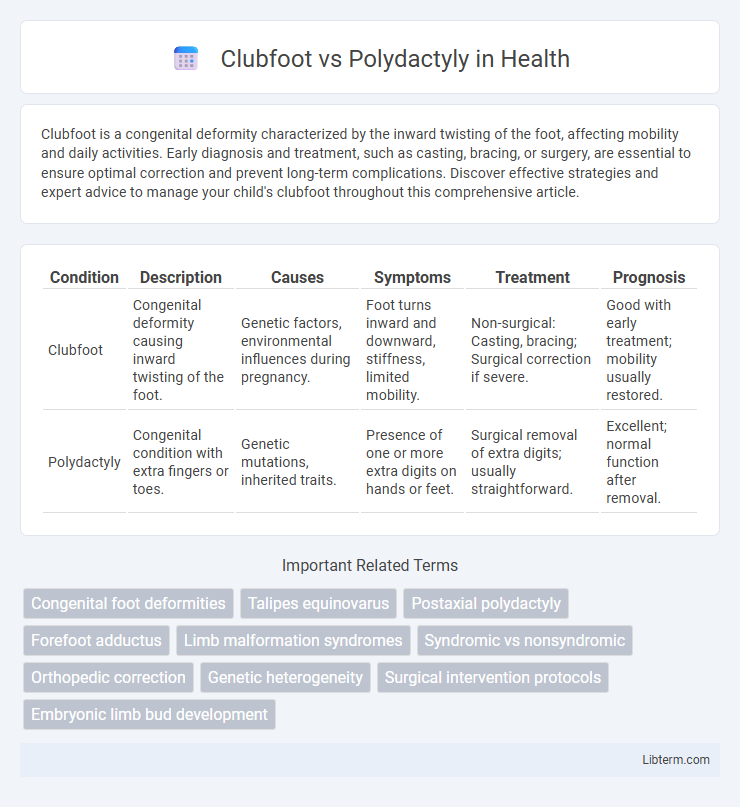
| Condition | Description | Causes | Symptoms | Treatment | Prognosis |
|---|---|---|---|---|---|
| Clubfoot | Congenital deformity causing inward twisting of the foot. | Genetic factors, environmental influences during pregnancy. | Foot turns inward and downward, stiffness, limited mobility. | Non-surgical: Casting, bracing; Surgical correction if severe. | Good with early treatment; mobility usually restored. |
| Polydactyly | Congenital condition with extra fingers or toes. | Genetic mutations, inherited traits. | Presence of one or more extra digits on hands or feet. | Surgical removal of extra digits; usually straightforward. | Excellent; normal function after removal. |
Introduction to Clubfoot and Polydactyly
Clubfoot, medically known as talipes equinovarus, is a congenital deformity characterized by the inward twisting of the foot, affecting approximately 1 in 1,000 live births worldwide. Polydactyly is a genetic condition marked by the presence of extra fingers or toes, occurring in about 1 in 500 to 1,000 births depending on the population. Both conditions are detectable at birth and require tailored medical assessment for optimal management and potential surgical intervention.
Causes and Genetic Factors
Clubfoot, medically known as congenital talipes equinovarus, primarily results from genetic mutations affecting musculoskeletal development combined with environmental factors such as intrauterine positioning. Polydactyly involves alterations in genes regulating limb patterning, notably mutations in the GLI3, ZRS, or SHH genes, leading to the presence of extra digits. Both conditions have hereditary components, but polydactyly often follows an autosomal dominant inheritance pattern, whereas clubfoot exhibits multifactorial inheritance involving several genes and environmental influences.
Clinical Presentation and Key Differences
Clubfoot presents as a congenital deformity characterized by inward twisting of the foot, restricted dorsiflexion, and a high arch, often diagnosed through physical examination at birth. Polydactyly involves the presence of extra fingers or toes, manifesting as distinct, fully or partially formed additional digits, which can be preaxial, postaxial, or central based on location. Key differences lie in clubfoot's musculoskeletal malalignment affecting foot mobility versus polydactyly's structural anomaly of digit number without impacting foot function.
Diagnosis and Screening Methods
Clubfoot diagnosis relies primarily on prenatal ultrasound, which detects the foot's abnormal inward position as early as 18-20 weeks of gestation, while postnatal clinical examination confirms foot rigidity and deformity. Polydactyly is often identified during routine prenatal ultrasound by visualizing extra digits, with genetic testing offering further insights into syndromic associations. Both conditions benefit from targeted imaging and genetic screening to guide early intervention and management strategies.
Epidemiology and Prevalence Rates
Clubfoot affects approximately 1 to 2 per 1,000 live births worldwide, with higher prevalence in males and certain ethnic groups such as Polynesians and Native Americans. Polydactyly occurs in about 1 in every 500 to 1,000 live births, more commonly seen in African populations and often inherited in an autosomal dominant pattern. Both conditions exhibit variable regional and genetic influences on their epidemiology, impacting diagnosis and treatment planning strategies.
Treatment Options for Clubfoot
Clubfoot treatment primarily involves non-surgical methods such as the Ponseti method, which includes gentle manipulation and serial casting to correct foot position. In more severe or resistant cases, surgical intervention may be necessary to release tendons and realign bones. Early diagnosis and treatment significantly improve outcomes, reducing the need for extensive surgery and enhancing mobility in affected infants.
Treatment Options for Polydactyly
Polydactyly treatment primarily involves surgical removal of the extra digit to improve hand or foot function and appearance, usually performed in early childhood. In some cases, minor splinting or physical therapy may be necessary post-surgery to ensure proper healing and mobility. Non-surgical interventions are rarely effective, making timely surgery the optimal approach for functional and cosmetic outcomes.
Prognosis and Long-term Outcomes
Clubfoot prognosis improves significantly with early intervention, such as the Ponseti method, resulting in over 90% of cases achieving functional, pain-free mobility without surgery. Polydactyly typically has an excellent long-term outcome following surgical removal of extra digits, with minimal impact on hand or foot function and aesthetics. Both conditions require timely management to optimize quality of life and reduce complications, but clubfoot may present ongoing challenges with rigidity or recurrence if treatment is delayed.
Psychosocial and Quality of Life Considerations
Clubfoot can lead to mobility challenges and social stigma, impacting self-esteem and limiting participation in physical activities, which may result in feelings of isolation and reduced quality of life. Polydactyly, while often less disabling, may cause psychosocial stress due to cosmetic concerns and social perception, particularly if untreated or visibly apparent. Both conditions require early intervention and supportive psychosocial care to enhance self-image and improve overall quality of life for affected individuals.
Recent Advances and Research Directions
Recent advances in clubfoot treatment emphasize minimally invasive techniques and the Ponseti method's enhanced protocols, improving long-term functional outcomes and reducing relapse rates. Genetic and molecular research in polydactyly explores the role of signaling pathways like Sonic Hedgehog (SHH) and GLI3 gene mutations, paving the way for potential gene therapy options. Emerging regenerative medicine approaches and 3D printing technologies are being investigated to correct complex deformities in both conditions with greater precision.
Clubfoot Infographic