Hypophosphatasia is a rare genetic disorder characterized by defective bone mineralization and low alkaline phosphatase activity, leading to weak bones and dental issues. Early diagnosis and tailored treatment can significantly improve quality of life by addressing symptoms and preventing complications. Discover how understanding Hypophosphatasia can empower your management and well-being in the full article.
Table of Comparison
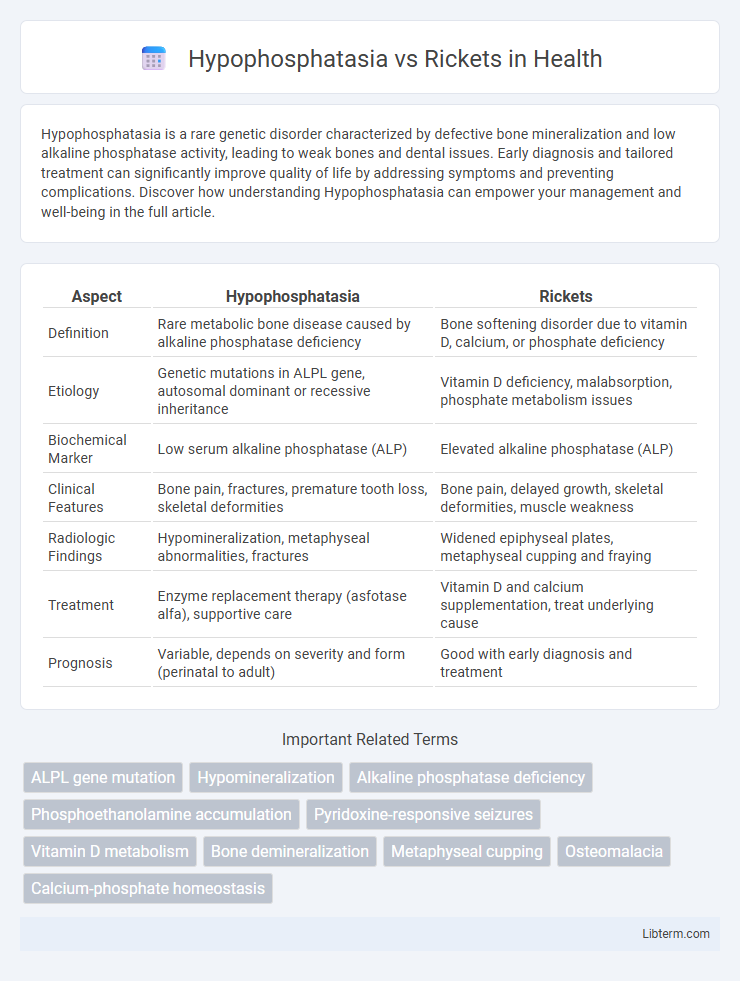
| Aspect | Hypophosphatasia | Rickets |
|---|---|---|
| Definition | Rare metabolic bone disease caused by alkaline phosphatase deficiency | Bone softening disorder due to vitamin D, calcium, or phosphate deficiency |
| Etiology | Genetic mutations in ALPL gene, autosomal dominant or recessive inheritance | Vitamin D deficiency, malabsorption, phosphate metabolism issues |
| Biochemical Marker | Low serum alkaline phosphatase (ALP) | Elevated alkaline phosphatase (ALP) |
| Clinical Features | Bone pain, fractures, premature tooth loss, skeletal deformities | Bone pain, delayed growth, skeletal deformities, muscle weakness |
| Radiologic Findings | Hypomineralization, metaphyseal abnormalities, fractures | Widened epiphyseal plates, metaphyseal cupping and fraying |
| Treatment | Enzyme replacement therapy (asfotase alfa), supportive care | Vitamin D and calcium supplementation, treat underlying cause |
| Prognosis | Variable, depends on severity and form (perinatal to adult) | Good with early diagnosis and treatment |
Introduction to Hypophosphatasia and Rickets
Hypophosphatasia is a rare metabolic bone disease characterized by defective mineralization due to mutations in the ALPL gene, leading to low alkaline phosphatase activity and accumulation of substrates like pyridoxal 5'-phosphate. Rickets primarily results from vitamin D deficiency, causing impaired calcium and phosphate metabolism, which weakens and softens bones in children. Both conditions manifest with skeletal abnormalities but differ significantly in their genetic causes, biochemical profiles, and treatment approaches.
Overview of Bone Metabolism Disorders
Hypophosphatasia is a rare genetic disorder characterized by defective mineralization of bones and teeth due to mutations in the ALPL gene, leading to low alkaline phosphatase activity, which disrupts bone metabolism. Rickets primarily results from vitamin D deficiency, causing impaired calcium and phosphate absorption, leading to soft and weakened bones in children. Both disorders affect bone mineralization but differ in pathophysiology, with hypophosphatasia involving enzymatic defects and rickets linked to nutritional or metabolic imbalances.
Causes of Hypophosphatasia
Hypophosphatasia is caused by mutations in the ALPL gene leading to deficient tissue-nonspecific alkaline phosphatase (TNSALP) activity, which disrupts bone mineralization and results in the accumulation of substrates like inorganic pyrophosphate. This genetic disorder contrasts with rickets, typically caused by vitamin D deficiency, calcium, or phosphate imbalance affecting bone development. The defective enzyme function in hypophosphatasia distinctly impairs hydroxyapatite formation, differentiating its pathophysiology from that of rickets.
Etiology of Rickets
Rickets is primarily caused by vitamin D deficiency, which leads to impaired calcium and phosphate metabolism and results in defective bone mineralization. Hypophosphatasia, on the other hand, is a genetic disorder characterized by mutations in the ALPL gene, causing deficient alkaline phosphatase activity and accumulation of inorganic pyrophosphate, inhibiting bone mineralization. The etiology of rickets involves nutritional deficits, malabsorption, or lack of sunlight exposure necessary for endogenous vitamin D synthesis.
Key Symptoms and Clinical Presentation
Hypophosphatasia presents with low alkaline phosphatase levels, premature loss of teeth, muscle weakness, and bone pain, often accompanied by skeletal abnormalities such as bowed limbs and fractures. In contrast, rickets typically manifests with bone deformities like wrist widening, rachitic rosary, delayed growth, and hypocalcemia-related symptoms due to vitamin D deficiency or phosphate metabolism disorders. Both conditions share symptoms of bone weakness, but hypophosphatasia is genetically linked to ALPL mutations affecting mineralization, while rickets results primarily from nutritional deficits or inheritance affecting vitamin D metabolism.
Diagnostic Criteria and Laboratory Findings
Hypophosphatasia is diagnosed through low serum alkaline phosphatase (ALP) levels, elevated urinary phosphoethanolamine, and genetic testing for ALPL gene mutations, distinguishing it from rickets which typically presents with normal or elevated ALP, low serum calcium, low phosphate, and increased parathyroid hormone (PTH). Radiographic findings in hypophosphatasia include poorly mineralized bone and metaphyseal abnormalities, while rickets shows widened growth plates and cupping of metaphyses due to defective mineralization from vitamin D deficiency. Laboratory findings such as low serum 25-hydroxyvitamin D and elevated alkaline phosphatase are characteristic of rickets but absent in hypophosphatasia, aiding in differential diagnosis.
Genetic Factors and Inheritance Patterns
Hypophosphatasia is caused by mutations in the ALPL gene leading to deficient tissue-nonspecific alkaline phosphatase, inherited in an autosomal recessive or dominant pattern depending on severity. Rickets primarily results from nutritional deficiencies but can also stem from genetic mutations affecting vitamin D metabolism or phosphate transport, often exhibiting X-linked or autosomal recessive inheritance. Genetic testing distinguishes hypophosphatasia from hereditary forms of rickets by identifying specific gene mutations responsible for abnormal bone mineralization.
Treatment Options and Management Strategies
Hypophosphatasia treatment focuses on enzyme replacement therapy with asfotase alfa to address alkaline phosphatase deficiency, while management includes pain control and physical therapy. Rickets treatment involves supplementation with vitamin D, calcium, and phosphate to correct mineral deficiencies and promote bone mineralization. Both conditions require multidisciplinary care to monitor growth, bone health, and prevent complications.
Prognosis and Long-Term Outlook
Hypophosphatasia prognosis varies widely based on disease severity, with infantile forms often leading to early mortality, while milder adult cases may experience chronic pain and fractures but normal lifespan. Rickets, primarily caused by vitamin D deficiency, generally has a favorable long-term outlook if treated early with supplementation, resulting in normal bone development and growth. Untreated rickets can cause permanent bone deformities and growth retardation, whereas hypophosphatasia may require ongoing management due to persistent metabolic abnormalities.
Preventive Measures and Patient Education
Preventive measures for Hypophosphatasia primarily involve early genetic counseling and monitoring alkaline phosphatase levels to detect enzyme deficiencies, while managing rickets focuses on ensuring adequate intake of vitamin D, calcium, and phosphate through diet and supplementation. Patient education for Hypophosphatasia emphasizes understanding the hereditary nature of the disorder and recognizing symptoms such as bone pain and dental issues, whereas education for rickets involves promoting exposure to sunlight and maintaining nutritional balance to prevent bone deformities. Both conditions require tailored guidance to reduce complications, improve bone health, and support long-term patient outcomes.
Hypophosphatasia Infographic