Factitious Disorder is a complex mental health condition where individuals deliberately produce or exaggerate symptoms of illness for psychological reasons rather than external incentives. This behavior can lead to unnecessary medical treatments and significant distress for both the person affected and healthcare providers. Discover how recognizing the signs and understanding the challenges of Factitious Disorder can help you support those impacted.
Table of Comparison
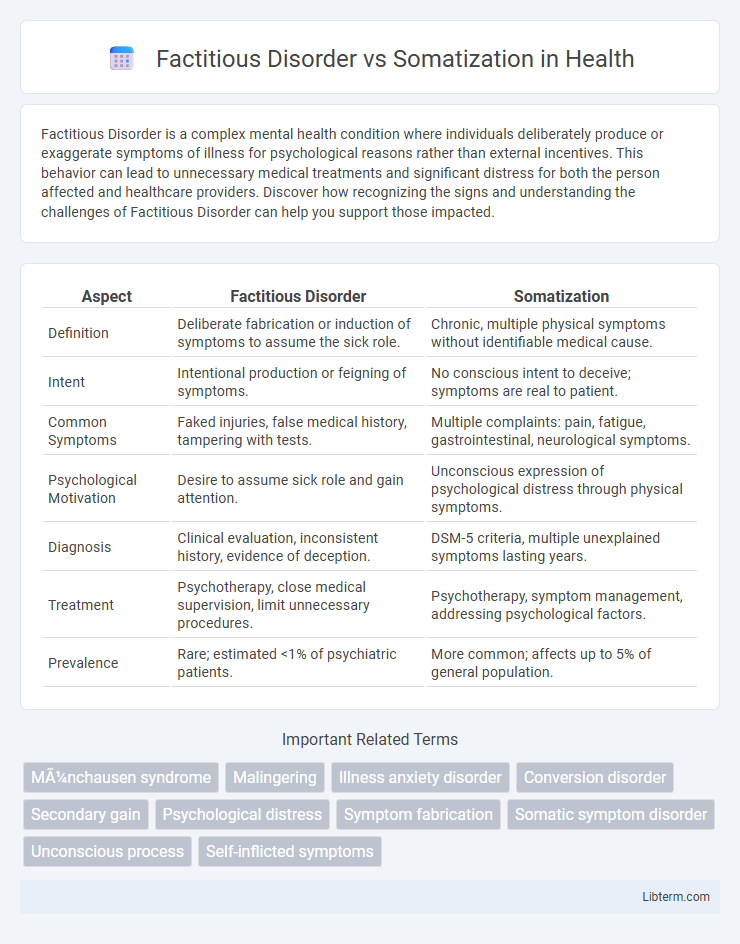
| Aspect | Factitious Disorder | Somatization |
|---|---|---|
| Definition | Deliberate fabrication or induction of symptoms to assume the sick role. | Chronic, multiple physical symptoms without identifiable medical cause. |
| Intent | Intentional production or feigning of symptoms. | No conscious intent to deceive; symptoms are real to patient. |
| Common Symptoms | Faked injuries, false medical history, tampering with tests. | Multiple complaints: pain, fatigue, gastrointestinal, neurological symptoms. |
| Psychological Motivation | Desire to assume sick role and gain attention. | Unconscious expression of psychological distress through physical symptoms. |
| Diagnosis | Clinical evaluation, inconsistent history, evidence of deception. | DSM-5 criteria, multiple unexplained symptoms lasting years. |
| Treatment | Psychotherapy, close medical supervision, limit unnecessary procedures. | Psychotherapy, symptom management, addressing psychological factors. |
| Prevalence | Rare; estimated <1% of psychiatric patients. | More common; affects up to 5% of general population. |
Understanding Factitious Disorder: Key Characteristics
Factitious disorder is characterized by the intentional fabrication or exaggeration of physical or psychological symptoms to assume the sick role without obvious external incentives, distinguishing it from somatization, where symptoms arise unconsciously and lack deliberate deception. Individuals with factitious disorder often engage in deceptive behaviors such as falsifying medical histories, manipulating test results, or self-inflicting injuries to produce symptoms. This disorder requires careful clinical assessment to differentiate it from somatization and other medical conditions, focusing on the motive behind symptom production and the absence of external gains like financial compensation.
Defining Somatization: An Overview
Somatization is a psychological phenomenon characterized by the presentation of physical symptoms that lack a medical explanation, frequently resulting from underlying emotional or psychological distress. This disorder involves multiple, recurring somatic complaints affecting various organ systems, often leading to significant impairment and frequent healthcare utilization. Unlike Factitious Disorder, where symptoms are intentionally fabricated or induced for psychological gain, somatization occurs without conscious deception, emphasizing the need for accurate diagnosis to guide effective treatment.
Core Differences Between Factitious Disorder and Somatization
Factitious Disorder involves intentional production or feigning of physical or psychological symptoms to assume the sick role, whereas Somatization refers to the chronic presence of multiple unexplained physical symptoms without conscious deception. Patients with Factitious Disorder deliberately falsify symptoms, often undergoing invasive procedures, while Somatization disorder manifests through persistent, medically unexplained complaints driven by psychological distress. Core differentiation hinges on the patient's motivation and awareness: Factitious Disorder is marked by intentional symptom fabrication, contrasting with the unconscious symptom reporting in Somatization.
Psychological Motivations: Factitious Disorder vs Somatization
Factitious Disorder involves a conscious psychological motivation to assume the sick role by intentionally producing or feigning symptoms, driven by a desire for attention or sympathy without external incentives. Somatization, in contrast, is characterized by unconscious psychological processes where individuals experience and report genuine physical symptoms without intentional fabrication or deception, often as an expression of emotional distress. Understanding these differing motivations is crucial for accurate diagnosis and tailored treatment strategies in clinical psychology.
Diagnostic Criteria: DSM-5 Perspectives
Factitious Disorder is characterized by intentional production or feigning of physical or psychological symptoms motivated by a desire to assume the sick role, without obvious external incentives, as outlined in DSM-5 criteria. Somatic Symptom Disorder involves one or more somatic symptoms causing distress or disruption, accompanied by excessive thoughts, feelings, or behaviors related to the symptoms, without deliberate fabrication. DSM-5 differentiates these conditions by emphasizing intentionality and the presence of external incentives in Factitious Disorder versus genuine symptom experience and psychological response in Somatic Symptom Disorder.
Common Symptoms and Clinical Presentations
Factitious Disorder and Somatization both involve physical symptoms without an identifiable medical cause, but Factitious Disorder is characterized by intentional fabrication or exaggeration of symptoms, often to assume the sick role. Common symptoms in Somatization include multiple, recurrent somatic complaints affecting various body systems, such as pain, gastrointestinal distress, and neurological symptoms, presenting in a chronic, non-deliberate manner. Clinical presentations in Factitious Disorder frequently involve dramatic but inconsistent symptom descriptions, frequent hospitalizations, and eagerness to undergo medical procedures, while Somatization displays persistent, medically unexplained symptoms with significant functional impairment but without conscious deception.
Assessment and Identification Techniques
Assessment of Factitious Disorder primarily involves thorough clinical interviews, corroborating patient history with medical records, and observing for deceptive behavior or symptom fabrication without external incentives. In contrast, Somatization Disorder assessment focuses on identifying multiple, recurrent somatic complaints unexplained by medical conditions, using standardized scales like the Patient Health Questionnaire-15 (PHQ-15) and structured clinical interviews such as the SCID-5. Differential identification relies on careful evaluation of symptom intentionality, with Factitious Disorder characterized by intentional feigning, while Somatization results from unconscious processes, necessitating multidisciplinary approaches including psychological evaluation and possible liaison psychiatry consultation.
Treatment Approaches for Factitious Disorder and Somatization
Treatment approaches for Factitious Disorder center on psychotherapy, particularly cognitive-behavioral therapy (CBT), to address underlying psychological motives and improve patient insight. Somatization disorder treatment typically involves a combination of regular medical care, cognitive-behavioral therapy to manage symptoms, and sometimes pharmacotherapy such as antidepressants. Both disorders benefit from a multidisciplinary approach involving mental health professionals and primary care providers to reduce unnecessary medical interventions and improve overall functioning.
Challenges in Clinical Management and Misdiagnosis
Factitious Disorder presents significant challenges in clinical management due to patients deliberately producing or feigning symptoms, complicating accurate diagnosis and treatment, while Somatization Disorder involves genuine physical symptoms without a clear medical cause, often leading to extensive and unnecessary medical investigations. Misdiagnosis occurs frequently as Factitious Disorder can be mistaken for genuine medical conditions, and Somatization symptoms are often attributed solely to psychological factors without thorough evaluation of potential organic causes. Effective management requires a multidisciplinary approach including psychiatric evaluation, careful clinical observation, and communication strategies to minimize unnecessary procedures and foster therapeutic alliance.
Impacts on Patients and Healthcare Systems
Factitious Disorder involves patients deliberately producing or feigning symptoms, leading to unnecessary medical tests and procedures that strain healthcare resources and increase costs. Somatization disorder causes patients to experience genuine, chronic physical symptoms without identifiable medical causes, resulting in frequent medical visits and extensive diagnostic evaluations that challenge healthcare providers. Both disorders impose significant psychological distress on patients and create complex case management scenarios that demand multidisciplinary approaches for effective treatment.
Factitious Disorder Infographic