Urolithiasis involves the formation of stones in the urinary tract, causing pain and urinary symptoms that require timely diagnosis and management. Bladder tumors, often detected through imaging or cystoscopy, can range from benign growths to malignant cancers needing precise intervention. Explore the following article to understand how to prevent, diagnose, and treat these urological conditions effectively for your health.
Table of Comparison
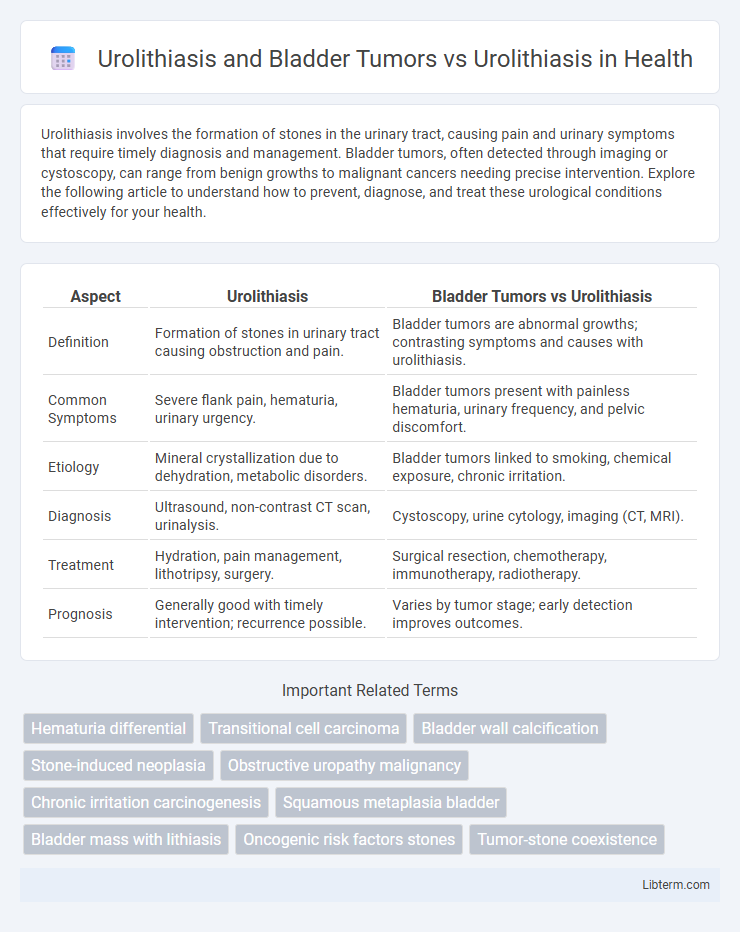
| Aspect | Urolithiasis | Bladder Tumors vs Urolithiasis |
|---|---|---|
| Definition | Formation of stones in urinary tract causing obstruction and pain. | Bladder tumors are abnormal growths; contrasting symptoms and causes with urolithiasis. |
| Common Symptoms | Severe flank pain, hematuria, urinary urgency. | Bladder tumors present with painless hematuria, urinary frequency, and pelvic discomfort. |
| Etiology | Mineral crystallization due to dehydration, metabolic disorders. | Bladder tumors linked to smoking, chemical exposure, chronic irritation. |
| Diagnosis | Ultrasound, non-contrast CT scan, urinalysis. | Cystoscopy, urine cytology, imaging (CT, MRI). |
| Treatment | Hydration, pain management, lithotripsy, surgery. | Surgical resection, chemotherapy, immunotherapy, radiotherapy. |
| Prognosis | Generally good with timely intervention; recurrence possible. | Varies by tumor stage; early detection improves outcomes. |
Overview of Urolithiasis
Urolithiasis refers to the formation of stones within the urinary tract, primarily in the kidneys, ureters, or bladder, caused by supersaturation of minerals such as calcium, oxalate, and uric acid. These renal calculi can cause severe pain, obstruction, and potential urinary tract infections, necessitating diagnostic imaging like ultrasound or CT scans for accurate detection. While urolithiasis primarily involves stone formation, bladder tumors represent abnormal cellular growth in the bladder lining, with distinct etiology and clinical implications unrelated to stone development.
Introduction to Bladder Tumors
Bladder tumors commonly arise due to abnormal cellular growth in the bladder lining, differentiating them from urolithiasis, which involves the formation of urinary stones within the urinary tract. The most prevalent type of bladder tumor is transitional cell carcinoma, accounting for over 90% of cases, with risk factors including smoking, chemical exposure, and chronic bladder irritation. Unlike urolithiasis, which primarily causes pain and hematuria through physical obstruction, bladder tumors often present with painless hematuria and require cystoscopic evaluation for accurate diagnosis.
Urolithiasis: Causes and Risk Factors
Urolithiasis, characterized by the formation of urinary stones, is primarily caused by metabolic imbalances such as hypercalciuria, hyperoxaluria, and low urine volume leading to supersaturation of stone-forming salts. Risk factors include dehydration, high dietary intake of oxalate or sodium, obesity, genetic predisposition, and certain medical conditions like gout and hyperparathyroidism. Unlike bladder tumors, which originate from abnormal cell growth in the bladder lining, urolithiasis involves physical obstruction and inflammation caused by stone formation within the urinary tract.
Bladder Tumors: Types and Pathogenesis
Bladder tumors primarily include urothelial carcinoma, squamous cell carcinoma, and adenocarcinoma, with urothelial carcinoma accounting for over 90% of cases. Their pathogenesis involves genetic mutations in oncogenes and tumor suppressor genes such as TP53 and FGFR3, alongside environmental factors like tobacco smoke and chronic irritation from urolithiasis. Chronic inflammation from urinary stones can contribute to malignant transformation by inducing cellular atypia and promoting a microenvironment conducive to tumorigenesis.
Clinical Presentation: Urolithiasis vs Bladder Tumors
Urolithiasis typically presents with acute flank pain, hematuria, and sometimes nausea or vomiting due to stone obstruction in the urinary tract. Bladder tumors more commonly manifest with painless gross hematuria, urinary frequency, and dysuria without the severe pain characteristic of stones. Differentiating these clinical presentations is crucial for accurate diagnosis and appropriate management.
Diagnostic Approaches: Differentiating Urolithiasis and Bladder Tumors
Accurate diagnosis of urolithiasis and bladder tumors relies on a combination of imaging techniques and laboratory tests, with non-contrast helical CT scans offering high sensitivity for detecting urinary stones while cystoscopy remains the gold standard for visualizing bladder tumors. Urinalysis and urine cytology provide critical information, identifying hematuria and malignant cells that guide differentiation between the two conditions. Advanced diagnostic tools like multiparametric MRI improve tissue characterization, aiding clinicians in distinguishing tumor masses from obstructive calculi in complex cases.
Imaging Findings: Stones vs Tumors in the Bladder
Imaging findings in urolithiasis primarily reveal hyperdense calcified stones within the bladder on non-contrast CT scans, often with posterior acoustic shadowing on ultrasound, indicating stone composition and size. In contrast, bladder tumors typically present as irregular, enhancing soft tissue masses on contrast-enhanced CT or MRI, with possible wall thickening and disrupted urothelial lining, distinguishing them from calcified stones. Differentiating these entities is critical for appropriate management, relying on the radiologic appearance of discrete calcifications versus enhancing masses in the bladder lumen.
Treatment Options: Urolithiasis Compared to Bladder Tumors
Treatment options for urolithiasis primarily include extracorporeal shock wave lithotripsy (ESWL), ureteroscopy with laser lithotripsy, and percutaneous nephrolithotomy, targeting the fragmentation and removal of kidney or urinary tract stones. In contrast, bladder tumors require treatments such as transurethral resection of bladder tumor (TURBT), intravesical chemotherapy or immunotherapy (e.g., Bacillus Calmette-Guerin), and radical cystectomy for invasive cancer. Unlike urolithiasis, bladder tumor therapy focuses on oncologic control and prevention of recurrence rather than stone clearance.
Prognosis and Potential Complications
Urolithiasis complicated by bladder tumors significantly worsens the prognosis compared to urolithiasis alone, with increased risks of hematuria, urinary obstruction, and infection. Potential complications include tumor progression leading to invasive bladder cancer and recurrence of stone formation due to altered bladder physiology. Early detection and integrated management of both conditions are critical to improve survival rates and reduce morbidity.
Importance of Early Detection and Differentiation
Early detection and accurate differentiation between urolithiasis and bladder tumors are critical for effective treatment and improved patient outcomes. Imaging techniques such as ultrasound, CT scans, and cystoscopy play a pivotal role in distinguishing these conditions, as symptoms like hematuria and urinary obstruction can overlap. Prompt diagnosis enables targeted therapy, reduces complications, and prevents mismanagement in cases presenting with similar clinical profiles.
Urolithiasis and Bladder Tumors Infographic