Hypernatremia occurs when there is an elevated sodium concentration in the blood, often due to dehydration or excessive sodium intake. This condition can lead to symptoms such as confusion, muscle twitching, and in severe cases, seizures or coma. Explore the rest of the article to understand the causes, symptoms, and treatment options for hypernatremia to protect your health.
Table of Comparison
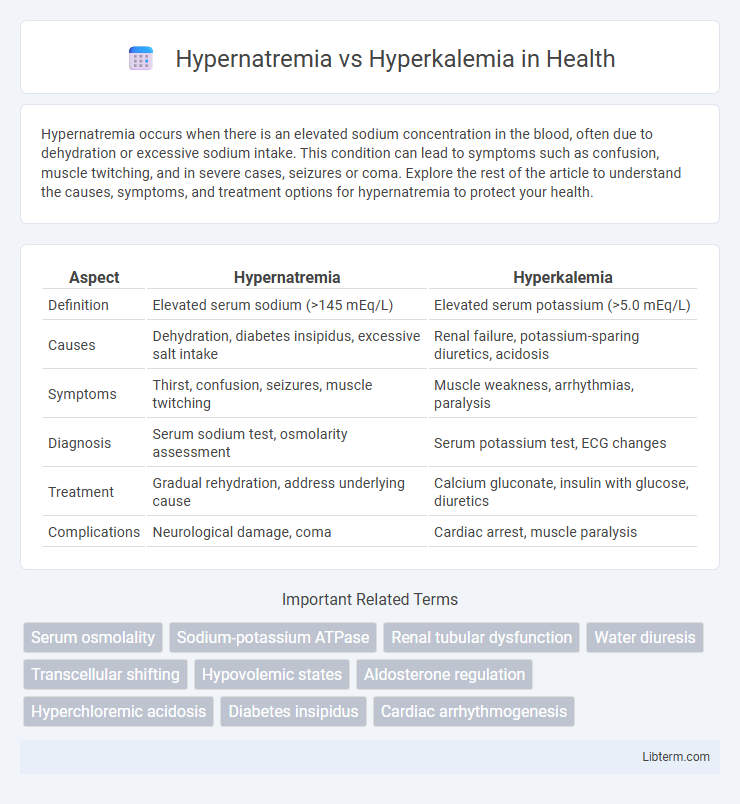
| Aspect | Hypernatremia | Hyperkalemia |
|---|---|---|
| Definition | Elevated serum sodium (>145 mEq/L) | Elevated serum potassium (>5.0 mEq/L) |
| Causes | Dehydration, diabetes insipidus, excessive salt intake | Renal failure, potassium-sparing diuretics, acidosis |
| Symptoms | Thirst, confusion, seizures, muscle twitching | Muscle weakness, arrhythmias, paralysis |
| Diagnosis | Serum sodium test, osmolarity assessment | Serum potassium test, ECG changes |
| Treatment | Gradual rehydration, address underlying cause | Calcium gluconate, insulin with glucose, diuretics |
| Complications | Neurological damage, coma | Cardiac arrest, muscle paralysis |
Introduction to Hypernatremia and Hyperkalemia
Hypernatremia is characterized by elevated sodium levels in the blood, typically exceeding 145 mEq/L, often resulting from dehydration, excessive sodium intake, or impaired kidney function. Hyperkalemia involves increased potassium levels above 5.0 mEq/L, commonly caused by renal failure, medications, or cellular injury disrupting potassium balance. Both electrolyte imbalances significantly affect cardiac and neurological function, necessitating prompt diagnosis and tailored treatment based on underlying etiologies.
Definition and Pathophysiology
Hypernatremia is defined as an elevated serum sodium concentration exceeding 145 mEq/L, resulting from water loss or sodium gain leading to cellular dehydration and neurologic symptoms. Hyperkalemia refers to a serum potassium level above 5.0 mEq/L, often caused by impaired renal excretion, excessive potassium intake, or cellular release, which disrupts cardiac and neuromuscular function through altered membrane potentials. Both conditions involve electrolyte imbalances but affect distinct ions with different mechanisms influencing cell excitability and fluid balance.
Causes of Hypernatremia
Hypernatremia primarily results from water loss exceeding sodium loss due to dehydration, diabetes insipidus, or insufficient water intake, while hyperkalemia stems from impaired potassium excretion, excessive potassium intake, or cellular shifts caused by conditions like renal failure or acidosis. Key causes of hypernatremia include excessive sweating, diarrhea, burns, or diuretic use leading to free water depletion. Understanding these pathophysiological mechanisms is crucial for accurate diagnosis and targeted management in electrolyte imbalance cases.
Causes of Hyperkalemia
Hyperkalemia commonly arises from kidney dysfunction, which impairs potassium excretion, leading to elevated serum potassium levels. Other primary causes include the use of potassium-sparing diuretics, adrenal insufficiency (such as Addison's disease), and cellular release of potassium due to tissue breakdown from conditions like rhabdomyolysis or hemolysis. Excessive potassium intake, acidosis, and certain medications such as ACE inhibitors or NSAIDs also contribute significantly to the development of hyperkalemia.
Clinical Manifestations: Comparing Symptoms
Hypernatremia typically presents with neurological symptoms such as confusion, lethargy, irritability, and seizures due to cellular dehydration and brain shrinkage. Hyperkalemia primarily affects cardiac function, leading to muscle weakness, paralysis, and life-threatening arrhythmias like peaked T waves, widening QRS complexes, or ventricular fibrillation observed on ECG. Recognizing the distinct clinical manifestations of hypernatremia versus hyperkalemia is crucial for prompt diagnosis and targeted treatment to prevent complications.
Diagnostic Approaches
Diagnostic approaches for hypernatremia involve measuring serum sodium levels above 145 mEq/L and assessing patient history for dehydration, diabetes insipidus, or excessive salt intake. Hyperkalemia diagnosis requires serum potassium levels exceeding 5.0 mEq/L, along with ECG evaluation for peaked T waves, widened QRS complexes, and laboratory tests to identify causes such as renal failure or medication effects. Accurate differentiation depends on comprehensive metabolic panels and clinical correlation of electrolyte imbalances with patient symptoms.
Laboratory Findings and Electrolyte Imbalances
Hypernatremia presents with elevated serum sodium levels above 145 mEq/L, often accompanied by hyperosmolality and signs of dehydration due to water loss exceeding sodium loss. Hyperkalemia is characterized by serum potassium levels exceeding 5.0 mEq/L, which can cause cardiac conduction abnormalities detectable on electrocardiograms, such as peaked T waves and widened QRS complexes. Both conditions require precise laboratory monitoring of electrolyte panels to identify imbalances, with hypernatremia reflecting sodium-water dysregulation and hyperkalemia indicating potassium retention often linked to renal impairment or cellular breakdown.
Treatment Strategies and Management
Treatment strategies for hypernatremia focus on gradual correction of serum sodium levels through controlled administration of hypotonic fluids and addressing the underlying cause of water loss or sodium gain. Management of hyperkalemia prioritizes stabilizing cardiac membranes with intravenous calcium gluconate, shifting potassium intracellularly using insulin and glucose, and removing excess potassium via diuretics, sodium polystyrene sulfonate, or dialysis. Both conditions require close monitoring of electrolyte levels and renal function to prevent complications and guide therapy adjustments.
Complications and Prognosis
Hypernatremia often leads to severe neurological complications such as seizures, coma, and permanent brain damage due to cellular dehydration and cerebral shrinkage. Hyperkalemia primarily causes life-threatening cardiac arrhythmias, including ventricular fibrillation and cardiac arrest, resulting from altered cardiac conduction and membrane potential. Prognosis for both depends on the severity and rapidity of onset; hyperkalemia has a higher risk of sudden death if untreated, whereas hypernatremia prognosis worsens with prolonged hyperosmolar states and underlying conditions.
Prevention and Patient Education
Preventing hypernatremia involves monitoring sodium intake, ensuring adequate hydration, and educating patients on recognizing early symptoms such as excessive thirst and confusion. Hyperkalemia prevention centers on managing potassium-rich diets, regulating medications like ACE inhibitors or potassium-sparing diuretics, and understanding signs such as muscle weakness or cardiac irregularities. Patient education should emphasize regular blood tests, adherence to prescribed dietary guidelines, and immediate reporting of symptoms to healthcare providers to reduce risks and complications associated with electrolyte imbalances.
Hypernatremia Infographic