Hypokalemia, characterized by low potassium levels in the blood, can cause muscle weakness, fatigue, and irregular heart rhythms. Proper diagnosis and treatment are essential to restore potassium balance and prevent serious complications. Discover effective strategies to manage hypokalemia and protect Your health by reading the full article.
Table of Comparison
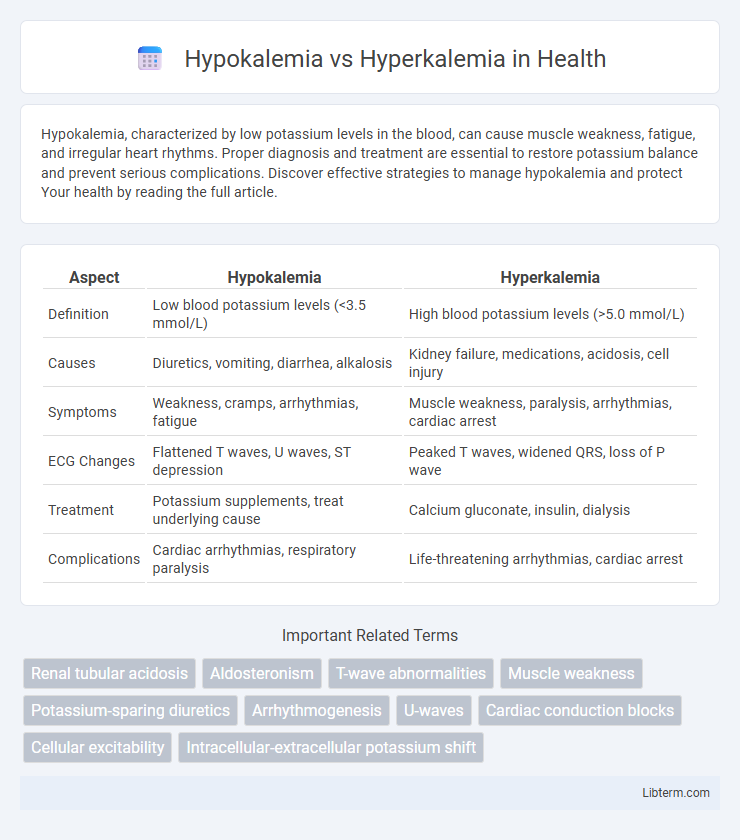
| Aspect | Hypokalemia | Hyperkalemia |
|---|---|---|
| Definition | Low blood potassium levels (<3.5 mmol/L) | High blood potassium levels (>5.0 mmol/L) |
| Causes | Diuretics, vomiting, diarrhea, alkalosis | Kidney failure, medications, acidosis, cell injury |
| Symptoms | Weakness, cramps, arrhythmias, fatigue | Muscle weakness, paralysis, arrhythmias, cardiac arrest |
| ECG Changes | Flattened T waves, U waves, ST depression | Peaked T waves, widened QRS, loss of P wave |
| Treatment | Potassium supplements, treat underlying cause | Calcium gluconate, insulin, dialysis |
| Complications | Cardiac arrhythmias, respiratory paralysis | Life-threatening arrhythmias, cardiac arrest |
Introduction to Potassium Imbalance
Potassium imbalance occurs when the body's potassium levels deviate from the normal range of 3.5 to 5.0 mEq/L, leading to conditions such as hypokalemia and hyperkalemia. Hypokalemia refers to low potassium levels below 3.5 mEq/L, often caused by factors like diuretic use, diarrhea, or inadequate intake, resulting in muscle weakness and cardiac arrhythmias. Hyperkalemia, on the other hand, involves elevated potassium levels above 5.0 mEq/L, commonly due to kidney failure, certain medications, or cellular injury, which can also trigger dangerous heart rhythm disturbances.
What is Hypokalemia?
Hypokalemia is a medical condition characterized by abnormally low levels of potassium in the blood, typically below 3.5 mEq/L. This electrolyte imbalance disrupts normal cellular function, potentially causing symptoms such as muscle weakness, cramps, fatigue, and cardiac arrhythmias. Common causes of hypokalemia include diuretic use, excessive vomiting or diarrhea, and certain endocrine disorders like hyperaldosteronism.
What is Hyperkalemia?
Hyperkalemia is a medical condition characterized by elevated levels of potassium in the blood, typically above 5.0 mmol/L. This electrolyte imbalance can disrupt normal cardiac and muscle function, leading to symptoms such as muscle weakness, fatigue, and dangerous cardiac arrhythmias. Causes of hyperkalemia include kidney failure, certain medications, and excessive potassium intake, requiring prompt medical evaluation and treatment to prevent complications.
Causes of Hypokalemia
Hypokalemia is primarily caused by excessive potassium loss through gastrointestinal disturbances such as vomiting or diarrhea, and renal losses due to diuretic use or certain kidney disorders. Other causes include inadequate potassium intake, shifts of potassium into cells triggered by insulin or alkalosis, and hormonal imbalances like hyperaldosteronism. Understanding these etiologies is crucial for distinguishing hypokalemia from hyperkalemia, which usually involves potassium retention or decreased excretion.
Causes of Hyperkalemia
Hyperkalemia is primarily caused by impaired renal excretion of potassium due to conditions such as acute kidney injury, chronic kidney disease, or the use of potassium-sparing diuretics and ACE inhibitors. Excessive potassium intake, cellular breakdown from trauma or hemolysis, and adrenal insufficiency leading to hypoaldosteronism also contribute significantly. Understanding these etiologies aids in differentiating hyperkalemia from hypokalemia, which involves low serum potassium levels often due to diuretics, gastrointestinal losses, or aldosterone excess.
Symptoms: Hypokalemia vs Hyperkalemia
Hypokalemia manifests with symptoms such as muscle weakness, cramps, fatigue, and cardiac arrhythmias including premature ventricular contractions and flattened T waves on ECG. Hyperkalemia presents with muscle weakness, paresthesia, and life-threatening cardiac disturbances like bradycardia, peaked T waves, and widened QRS complexes on ECG. Both conditions require prompt diagnosis and electrolyte management to prevent severe neuromuscular and cardiovascular complications.
Diagnosis and Laboratory Findings
Hypokalemia is diagnosed by serum potassium levels below 3.5 mEq/L, often accompanied by alkalosis, hypomagnesemia, and elevated bicarbonate, while hyperkalemia presents with serum potassium levels above 5.0 mEq/L, often associated with metabolic acidosis and renal impairment. Electrocardiogram (ECG) changes in hypokalemia include U waves and flattened T waves, whereas hyperkalemia typically shows peaked T waves, widened QRS complexes, and potential sine wave patterns. Laboratory evaluation should include serum electrolytes, renal function tests, and arterial blood gas analysis to differentiate underlying causes and guide appropriate treatment.
Treatment Strategies for Hypokalemia
Treatment strategies for hypokalemia primarily involve potassium supplementation through oral or intravenous routes depending on severity, alongside addressing underlying causes such as diuretic use or gastrointestinal losses. Monitoring serum potassium levels and cardiac function is crucial to prevent complications like arrhythmias during correction. Adjusting medications that contribute to potassium depletion and ensuring adequate dietary potassium intake are also vital components of effective management.
Treatment Strategies for Hyperkalemia
Hyperkalemia treatment strategies prioritize stabilizing cardiac membranes with intravenous calcium gluconate, shifting potassium intracellularly using insulin and glucose, and promoting potassium elimination via diuretics, sodium polystyrene sulfonate, or dialysis. Continuous ECG monitoring is crucial to detect arrhythmias promptly during intervention. Unlike hypokalemia, which requires potassium supplementation, hyperkalemia management focuses on rapid potassium reduction to prevent life-threatening complications.
Prevention and Management Tips
Maintaining balanced potassium levels involves dietary modification, such as increasing intake of potassium-rich foods like bananas and spinach to prevent hypokalemia or limiting these foods to avoid hyperkalemia. Regular monitoring of serum potassium and kidney function is essential for early detection and management, especially in patients on diuretics or ACE inhibitors. Prompt treatment includes potassium supplementation for hypokalemia and potassium binders or dialysis for hyperkalemia, alongside addressing underlying causes.
Hypokalemia Infographic