Hypernatremia occurs when there is an excessive concentration of sodium in the blood, often due to dehydration or impaired kidney function. This electrolyte imbalance can cause symptoms ranging from thirst and confusion to seizures and coma if left untreated. Discover effective strategies for prevention and treatment by reading the rest of the article.
Table of Comparison
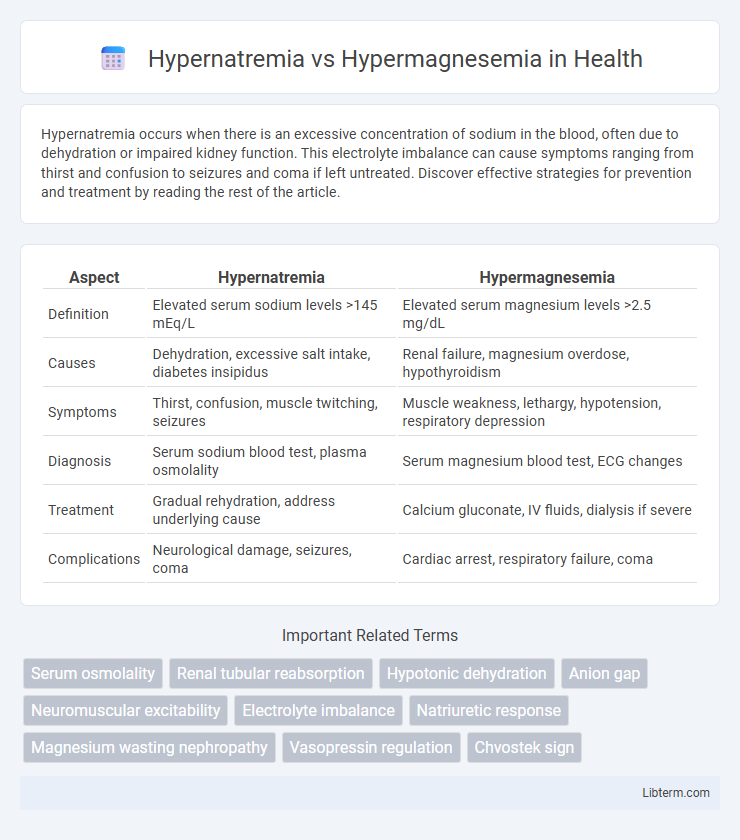
| Aspect | Hypernatremia | Hypermagnesemia |
|---|---|---|
| Definition | Elevated serum sodium levels >145 mEq/L | Elevated serum magnesium levels >2.5 mg/dL |
| Causes | Dehydration, excessive salt intake, diabetes insipidus | Renal failure, magnesium overdose, hypothyroidism |
| Symptoms | Thirst, confusion, muscle twitching, seizures | Muscle weakness, lethargy, hypotension, respiratory depression |
| Diagnosis | Serum sodium blood test, plasma osmolality | Serum magnesium blood test, ECG changes |
| Treatment | Gradual rehydration, address underlying cause | Calcium gluconate, IV fluids, dialysis if severe |
| Complications | Neurological damage, seizures, coma | Cardiac arrest, respiratory failure, coma |
Introduction to Hypernatremia and Hypermagnesemia
Hypernatremia is a condition characterized by elevated sodium levels in the blood, typically exceeding 145 mmol/L, resulting from water loss or excessive sodium intake. Hypermagnesemia involves abnormally high magnesium concentrations above 2.5 mg/dL, often due to impaired renal excretion or magnesium supplementation. Both electrolyte imbalances disrupt cellular function and require precise diagnosis for effective management.
Definition and Overview
Hypernatremia is a condition characterized by elevated sodium levels in the blood, typically exceeding 145 mEq/L, leading to cellular dehydration and neurological symptoms. Hypermagnesemia involves an increased concentration of magnesium in the bloodstream, usually above 2.5 mg/dL, often resulting from kidney dysfunction or excessive magnesium intake. Both conditions require accurate diagnosis and management to prevent severe complications related to electrolyte imbalance.
Etiology and Risk Factors
Hypernatremia primarily results from excessive sodium intake, dehydration, or impaired renal water excretion, commonly seen in elderly patients, infants, and those with impaired thirst mechanisms. Hypermagnesemia is often caused by renal failure, excessive magnesium-containing medications or supplements, and adrenal insufficiency, with risk factors including chronic kidney disease and overuse of magnesium-based antacids or laxatives. Both conditions frequently occur in hospitalized or critically ill patients due to disrupted electrolyte homeostasis and comorbidities.
Pathophysiology Comparison
Hypernatremia results from an imbalance in sodium and water homeostasis causing increased plasma sodium concentration, often due to water loss or sodium gain, leading to cellular dehydration and impaired neurological function. Hypermagnesemia arises from excessive magnesium accumulation, primarily due to renal insufficiency or magnesium overdose, causing neuromuscular and cardiovascular depression through calcium channel blockade and decreased acetylcholine release. Both conditions disrupt electrolyte balance but distinctly affect cellular mechanisms: hypernatremia alters osmotic gradients causing cellular shrinkage, while hypermagnesemia directly inhibits synaptic transmission and muscle contraction.
Clinical Manifestations
Hypernatremia presents with clinical manifestations such as intense thirst, dry mucous membranes, restlessness, and neurological symptoms including confusion, seizures, and coma due to cellular dehydration, particularly in brain cells. In contrast, hypermagnesemia commonly exhibits symptoms like hypotension, diminished deep tendon reflexes, muscle weakness, and respiratory depression, resulting from excessive magnesium's depressant effect on neuromuscular and cardiovascular function. Both electrolyte imbalances require prompt diagnosis and management to prevent severe complications and improve patient outcomes.
Diagnostic Approaches
Hypernatremia diagnosis relies primarily on serum sodium measurements exceeding 145 mEq/L, combined with clinical assessment of hydration status and osmolality tests to evaluate water balance. Hypermagnesemia is identified through elevated serum magnesium levels above 2.5 mg/dL, often confirmed with renal function tests and electrolyte panels to detect underlying causes such as renal insufficiency or magnesium overdose. Both conditions require targeted laboratory investigations including arterial blood gases for acid-base status and urine studies to determine electrolyte excretion abnormalities.
Management and Treatment Strategies
Management of hypernatremia prioritizes gradual correction of serum sodium levels using hypotonic fluids or free water administration to prevent cerebral edema, with close monitoring of electrolyte balance and renal function. Treatment of hypermagnesemia involves cessation of exogenous magnesium sources, intravenous calcium gluconate to antagonize cardiac and neuromuscular effects, and promoting magnesium excretion via intravenous fluids and loop diuretics; severe cases may require hemodialysis. Both conditions necessitate tailored interventions based on severity, presenting symptoms, and underlying etiologies to restore electrolyte homeostasis effectively.
Complications and Prognosis
Hypernatremia often leads to severe neurological complications such as seizures, coma, and irreversible brain damage due to cellular dehydration, significantly increasing mortality risk if untreated. Hypermagnesemia primarily causes cardiovascular complications including hypotension, bradycardia, and respiratory depression, with prognosis worsening in cases of renal failure or delayed intervention. Early diagnosis and management of electrolyte imbalances are critical for improving patient outcomes and preventing long-term sequelae in both conditions.
Prevention and Patient Education
Preventing hypernatremia involves educating patients on maintaining adequate hydration, especially during illness or heat exposure, and monitoring sodium intake in individuals with kidney or cardiac conditions. For hypermagnesemia prevention, patient education should emphasize avoiding excessive magnesium-containing medications, such as antacids and laxatives, particularly in those with impaired renal function. Both conditions require regular monitoring of electrolyte levels and prompt medical consultation when symptoms like confusion, muscle weakness, or irregular heartbeat arise.
Summary and Key Takeaways
Hypernatremia is characterized by elevated sodium levels above 145 mEq/L, often caused by dehydration or excessive sodium intake, leading to symptoms such as confusion, seizures, and muscle twitching. Hypermagnesemia occurs when magnesium levels exceed 2.5 mEq/L, usually due to renal failure or excessive magnesium administration, resulting in muscle weakness, hypotension, and respiratory depression. Effective management requires accurate diagnosis through serum electrolyte measurement and prompt correction of electrolyte imbalances to prevent severe neurological and cardiovascular complications.
Hypernatremia Infographic