Anisocoria is a condition characterized by unequal pupil sizes, which may indicate underlying neurological or ocular issues. Identifying the cause is crucial for appropriate treatment, as it can range from benign variations to serious medical conditions. Explore the article to learn how anisocoria can affect your eye health and when to seek professional care.
Table of Comparison
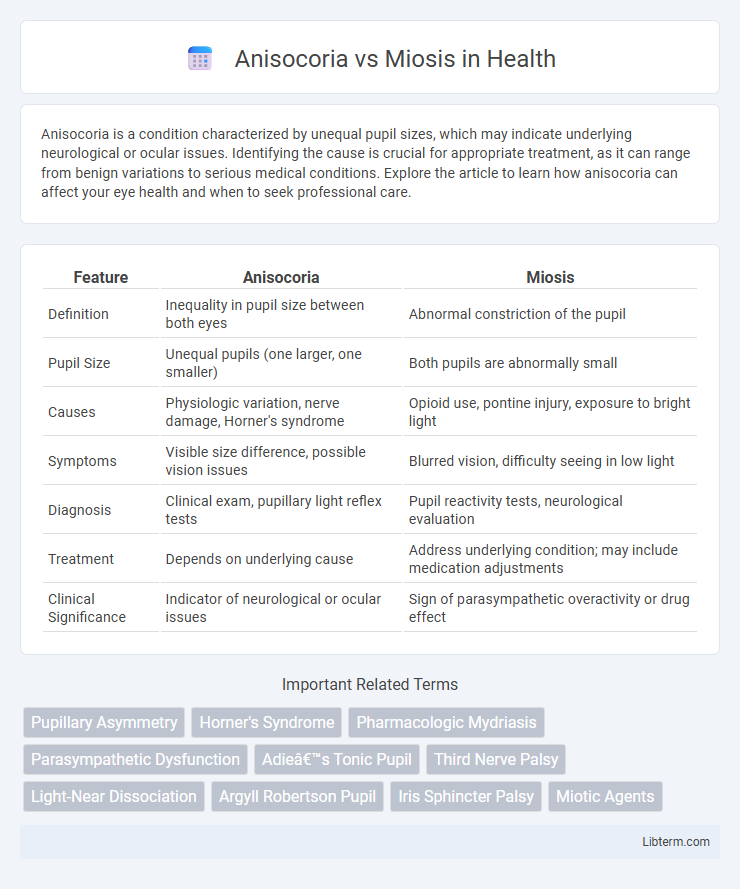
| Feature | Anisocoria | Miosis |
|---|---|---|
| Definition | Inequality in pupil size between both eyes | Abnormal constriction of the pupil |
| Pupil Size | Unequal pupils (one larger, one smaller) | Both pupils are abnormally small |
| Causes | Physiologic variation, nerve damage, Horner's syndrome | Opioid use, pontine injury, exposure to bright light |
| Symptoms | Visible size difference, possible vision issues | Blurred vision, difficulty seeing in low light |
| Diagnosis | Clinical exam, pupillary light reflex tests | Pupil reactivity tests, neurological evaluation |
| Treatment | Depends on underlying cause | Address underlying condition; may include medication adjustments |
| Clinical Significance | Indicator of neurological or ocular issues | Sign of parasympathetic overactivity or drug effect |
Understanding Anisocoria: Definition and Causes
Anisocoria refers to a condition characterized by unequal pupil sizes, which can result from physiological variations or underlying neurological disorders. Common causes include Horner's syndrome, third cranial nerve palsy, or localized eye trauma, each affecting the autonomic control of the iris muscles differently. Distinguishing anisocoria from miosis, which specifically denotes abnormally constricted pupils, is crucial for accurate diagnosis and targeted treatment.
What is Miosis? Key Characteristics Explained
Miosis is the medical term for excessive constriction of the pupil, resulting in a smaller pupil size that restricts light entry into the eye. Key characteristics of miosis include a pupil diameter less than 2 millimeters, unresponsiveness or sluggish reaction to light, and association with conditions such as opioid use, Horner's syndrome, or exposure to certain toxins. Unlike anisocoria, which involves unequal pupil sizes, miosis specifically refers to abnormally small pupils, often indicating underlying neurological or pharmacological causes.
Physiological vs. Pathological Pupillary Differences
Anisocoria refers to a condition where there is a significant difference in pupil sizes between the two eyes, which can be physiological in up to 20% of the population or pathological due to conditions like Horner's syndrome or third nerve palsy. Miosis, characterized by abnormally constricted pupils, is typically pathological when caused by factors such as opioid intoxication, pontine lesions, or exposure to cholinergic agents, but can also be physiological in response to bright light. Differentiating physiological from pathological pupillary differences relies on clinical context, presence of associated neurological signs, and pupillary light reflex assessment.
Clinical Presentation: How Anisocoria and Miosis Appear
Anisocoria presents as an unequal pupil size between the two eyes, which may be more noticeable in dim or bright lighting depending on the underlying cause, while miosis is characterized by an abnormally constricted pupil in one or both eyes. In anisocoria, the difference in pupil size can be transient or persistent and is often accompanied by other neurological signs such as ptosis or impaired eye movements. Clinical examination of miosis reveals a pinpoint pupil that reacts sluggishly or normally to light, commonly associated with opioid use, Horner's syndrome, or exposure to certain toxins.
Neurological Implications of Anisocoria
Anisocoria, characterized by unequal pupil sizes, often signals underlying neurological issues such as cranial nerve III palsy, Horner's syndrome, or intracranial pressure abnormalities. Miosis, the constriction of pupils, typically results from parasympathetic overactivity or opioid use but is less indicative of acute neurological damage. Identifying anisocoria in clinical settings requires urgent evaluation to rule out life-threatening conditions like aneurysms or brain herniation.
Common Causes and Triggers of Miosis
Miosis, characterized by excessive constriction of the pupils, often results from exposure to opioids, organophosphate poisoning, or certain neurological disorders such as Horner's syndrome. In contrast, anisocoria is the condition of unequal pupil sizes and can be caused by trauma, third nerve palsy, or pharmacologic agents that differentially affect the pupils. Understanding the triggers of miosis, including opioid overdose and parasympathetic activation, is crucial for accurate diagnosis and management.
Diagnostic Approaches: Differentiating Anisocoria from Miosis
Anisocoria is characterized by unequal pupil sizes, whereas miosis specifically refers to abnormally constricted pupils. Diagnostic approaches to differentiate anisocoria from miosis include detailed pupil size measurement under varied lighting conditions and pharmacologic testing with agents like cocaine or pilocarpine. Imaging studies such as MRI or CT scans may be employed to identify underlying neurological causes when anisocoria presents with additional symptoms.
Associated Symptoms and Red Flag Signs
Anisocoria, characterized by unequal pupil sizes, often presents with associated symptoms including ptosis, blurred vision, headache, or eye pain, which may indicate underlying neurological issues such as Horner's syndrome or third cranial nerve palsy. Miosis, defined as abnormally constricted pupils, is frequently accompanied by drooping eyelids and reduced light reflex, potentially signaling opioid intoxication, brainstem injury, or exposure to organophosphates. Red flag signs in both conditions include sudden onset, severe headache, vision changes, or systemic symptoms, necessitating urgent medical evaluation to rule out life-threatening causes like aneurysm rupture or stroke.
Treatment Strategies for Pupillary Disorders
Treatment strategies for anisocoria depend on its underlying cause, such as trauma, neurological disorders, or pharmacologic effects, often involving observation, medication, or surgical intervention if associated with serious conditions like Horner's syndrome or third nerve palsy. Miosis treatment focuses on addressing the cause, including atropine drops for drug-induced excessive constriction or managing opioid overdose with naloxone to reverse pinpoint pupils. Accurate diagnosis and targeted therapy are essential in managing pupillary disorders to restore normal pupil function and prevent complications.
Prognosis and When to Seek Medical Attention
Anisocoria, characterized by unequal pupil sizes, often has a benign prognosis when caused by physiological factors but may indicate serious neurological conditions such as Horner's syndrome or third nerve palsy requiring immediate medical evaluation. Miosis, or abnormally constricted pupils, typically results from exposure to opioids, medications, or neurological disorders like pontine hemorrhage, and its prognosis depends on addressing the underlying cause promptly. Seek emergency medical attention if anisocoria or miosis presents suddenly, worsens, or is accompanied by symptoms like vision changes, headache, or drooping eyelids to rule out life-threatening conditions.
Anisocoria Infographic