Renal cell carcinoma is the most common type of kidney cancer, originating in the lining of the small tubes within the kidney. Tumors often present symptoms like blood in the urine, flank pain, or a palpable mass, though early stages can be asymptomatic. Discover effective strategies for diagnosis, treatment options, and supportive care by exploring the rest of this article.
Table of Comparison
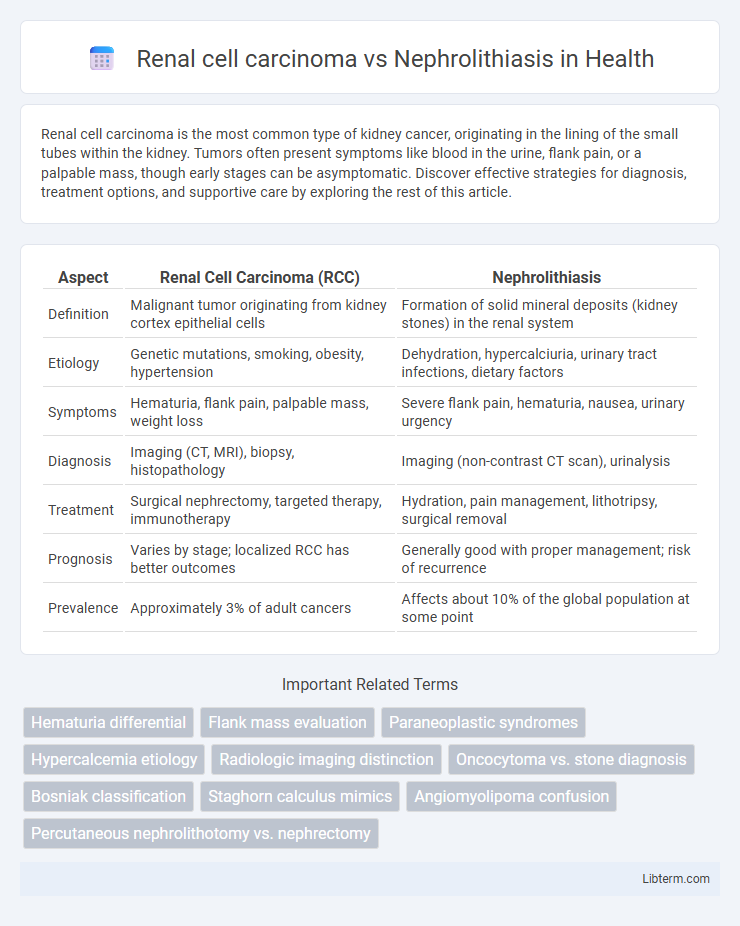
| Aspect | Renal Cell Carcinoma (RCC) | Nephrolithiasis |
|---|---|---|
| Definition | Malignant tumor originating from kidney cortex epithelial cells | Formation of solid mineral deposits (kidney stones) in the renal system |
| Etiology | Genetic mutations, smoking, obesity, hypertension | Dehydration, hypercalciuria, urinary tract infections, dietary factors |
| Symptoms | Hematuria, flank pain, palpable mass, weight loss | Severe flank pain, hematuria, nausea, urinary urgency |
| Diagnosis | Imaging (CT, MRI), biopsy, histopathology | Imaging (non-contrast CT scan), urinalysis |
| Treatment | Surgical nephrectomy, targeted therapy, immunotherapy | Hydration, pain management, lithotripsy, surgical removal |
| Prognosis | Varies by stage; localized RCC has better outcomes | Generally good with proper management; risk of recurrence |
| Prevalence | Approximately 3% of adult cancers | Affects about 10% of the global population at some point |
Introduction to Renal Cell Carcinoma and Nephrolithiasis
Renal cell carcinoma (RCC) is a malignant tumor originating from the renal cortex of the kidney, representing approximately 90% of adult kidney cancers with a strong association to smoking, obesity, and hypertension. Nephrolithiasis, commonly known as kidney stones, involves the formation of crystalline mineral concretions within the renal collecting system, causing severe flank pain and potential urinary obstruction. Understanding the distinct pathophysiological mechanisms and clinical presentations of RCC and nephrolithiasis is essential for accurate diagnosis and effective treatment strategies.
Epidemiology and Risk Factors
Renal cell carcinoma (RCC) primarily affects adults aged 50-70, with a higher incidence in males and a strong association with smoking, obesity, and hypertension. Nephrolithiasis occurs across all age groups but peaks between 30-60 years, with risk factors including dehydration, high dietary sodium, and metabolic disorders such as hypercalciuria. Both conditions show geographic variation, with RCC more prevalent in Western countries and nephrolithiasis common in hot climates promoting stone formation due to increased urine concentration.
Pathophysiology: RCC vs Nephrolithiasis
Renal cell carcinoma (RCC) arises from malignant transformation of renal tubular epithelial cells, often driven by genetic mutations such as VHL gene inactivation leading to VEGF-mediated angiogenesis and tumor proliferation. In contrast, nephrolithiasis involves the formation of crystalline aggregates due to supersaturation of urine with minerals like calcium oxalate or uric acid, causing obstruction and renal tissue injury. RCC pathophysiology is characterized by tumor growth and metastasis, whereas nephrolithiasis primarily results in mechanical damage and inflammation from stone obstruction.
Clinical Presentation and Symptoms
Renal cell carcinoma typically presents with hematuria, flank pain, and a palpable abdominal mass, while nephrolithiasis is most commonly characterized by sudden, severe flank pain radiating to the groin, hematuria, and urinary frequency or urgency. Patients with renal cell carcinoma may also experience systemic symptoms such as unexplained weight loss, fever, and night sweats, which are uncommon in nephrolithiasis. Nephrolithiasis symptoms often include nausea and vomiting due to acute pain, whereas renal cell carcinoma's presentation tends to be more insidious and may be discovered incidentally during imaging for unrelated issues.
Diagnostic Approaches and Imaging Techniques
Renal cell carcinoma (RCC) diagnosis primarily relies on imaging techniques such as contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI), which provide detailed visualization of renal masses and aid in tumor staging. Nephrolithiasis detection frequently employs non-contrast CT scans due to their high sensitivity for identifying urinary calculi, while ultrasound serves as a radiation-free alternative, especially in pregnant patients or those requiring repeated examinations. Differentiating RCC from nephrolithiasis involves recognizing characteristic imaging features, with RCC showing solid enhancing masses and nephrolithiasis presenting as hyperdense calculi within the urinary tract.
Key Differences in Laboratory Findings
Renal cell carcinoma typically presents with elevated erythrocyte sedimentation rate (ESR) and hypercalcemia due to paraneoplastic syndromes, whereas nephrolithiasis is often associated with normal calcium levels or hypercalciuria depending on stone composition. In renal cell carcinoma, urinalysis may show hematuria without infection, while nephrolithiasis frequently reveals microscopic or gross hematuria alongside crystalluria. Tumor markers are not standard diagnostic tools in nephrolithiasis, but imaging combined with abnormal lab values like increased lactate dehydrogenase (LDH) can support suspicion of renal cell carcinoma.
Complications: Malignant vs Benign Outcomes
Renal cell carcinoma (RCC) presents malignant complications such as local tissue invasion, metastasis to lungs, bones, and lymph nodes, and potential paraneoplastic syndromes, significantly impacting prognosis and treatment strategies. Nephrolithiasis, a benign condition characterized by kidney stones, primarily leads to complications including urinary tract obstruction, recurrent infections, and potential kidney damage or loss of function without the systemic spread seen in RCC. Distinguishing these outcomes is critical, as RCC requires oncologic management, whereas nephrolithiasis often involves pain control and stone removal with usually favorable long-term outcomes.
Treatment Strategies and Management Options
Treatment strategies for Renal Cell Carcinoma (RCC) primarily involve surgical intervention such as partial or radical nephrectomy, along with targeted therapies including tyrosine kinase inhibitors for advanced stages. In contrast, Nephrolithiasis management focuses on stone removal techniques like extracorporeal shock wave lithotripsy (ESWL), ureteroscopy, and percutaneous nephrolithotomy, combined with preventive measures such as hydration and dietary modifications. Both conditions require tailored approaches based on disease severity, with RCC emphasizing oncologic control and Nephrolithiasis prioritizing symptomatic relief and recurrence prevention.
Prognosis and Long-Term Outcomes
Renal cell carcinoma (RCC) typically presents a variable prognosis depending on the tumor stage and grade, with localized RCC showing a five-year survival rate exceeding 70%, while metastatic disease has significantly poorer outcomes. Nephrolithiasis, or kidney stones, generally has an excellent long-term prognosis with appropriate treatment, though recurrent stones may lead to chronic kidney disease and associated complications. Early diagnosis and management are critical for RCC to improve survival rates, whereas preventive strategies play a key role in minimizing nephrolithiasis recurrence and preserving renal function.
Prevention and Patient Education
Renal cell carcinoma prevention emphasizes avoiding smoking, managing hypertension, and maintaining a healthy weight to reduce cancer risk. Nephrolithiasis prevention involves adequate hydration, dietary modifications such as limiting sodium and oxalate intake, and monitoring calcium levels to prevent kidney stone formation. Patient education should focus on lifestyle changes, symptom recognition, and adherence to medical advice to improve outcomes for both conditions.
Renal cell carcinoma Infographic