Ascites is the abnormal accumulation of fluid in the abdominal cavity, often caused by liver disease, heart failure, or cancer. This condition can lead to discomfort, swelling, and difficulty breathing, requiring prompt medical evaluation and treatment options tailored to the underlying cause. Discover more about ascites symptoms, causes, and effective management strategies in the rest of this article.
Table of Comparison
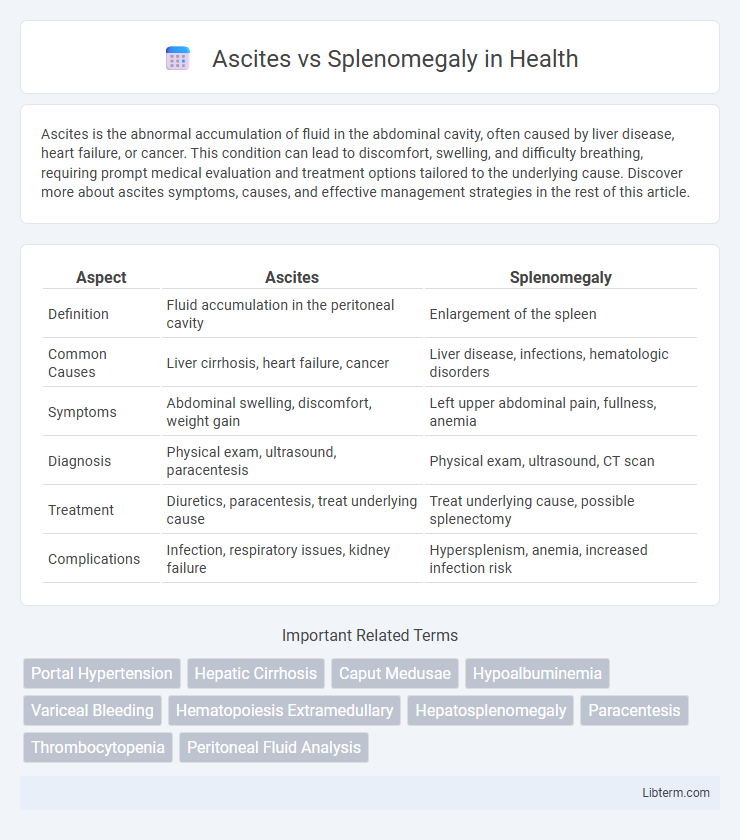
| Aspect | Ascites | Splenomegaly |
|---|---|---|
| Definition | Fluid accumulation in the peritoneal cavity | Enlargement of the spleen |
| Common Causes | Liver cirrhosis, heart failure, cancer | Liver disease, infections, hematologic disorders |
| Symptoms | Abdominal swelling, discomfort, weight gain | Left upper abdominal pain, fullness, anemia |
| Diagnosis | Physical exam, ultrasound, paracentesis | Physical exam, ultrasound, CT scan |
| Treatment | Diuretics, paracentesis, treat underlying cause | Treat underlying cause, possible splenectomy |
| Complications | Infection, respiratory issues, kidney failure | Hypersplenism, anemia, increased infection risk |
Introduction to Ascites and Splenomegaly
Ascites is the abnormal accumulation of fluid in the peritoneal cavity, commonly caused by liver cirrhosis, heart failure, or malignancies, leading to abdominal distension and discomfort. Splenomegaly refers to the enlargement of the spleen due to infections, hematologic diseases, or portal hypertension, often presenting with left upper quadrant pain or hypersplenism. Differentiating ascites and splenomegaly relies on clinical examination and imaging, crucial for accurate diagnosis and targeted treatment.
Definitions: What is Ascites? What is Splenomegaly?
Ascites is the abnormal accumulation of fluid in the peritoneal cavity, often caused by liver cirrhosis, cancer, or heart failure. Splenomegaly refers to the enlargement of the spleen, frequently resulting from infections, liver diseases, or hematologic disorders. Both conditions are critical clinical findings used to diagnose and assess underlying systemic diseases.
Etiology: Causes of Ascites vs Causes of Splenomegaly
Ascites primarily results from liver cirrhosis, heart failure, malignancies, and infections such as tuberculosis or peritonitis, causing fluid accumulation in the peritoneal cavity. Splenomegaly is commonly caused by hematologic disorders like leukemia and lymphoma, infections including mononucleosis and malaria, and portal hypertension secondary to liver disease. While ascites is mainly related to fluid imbalance and vascular pressure changes, splenomegaly arises due to increased demand for splenic filtration or infiltration by abnormal cells.
Pathophysiology: How Ascites and Splenomegaly Develop
Ascites develops primarily due to portal hypertension, causing increased hydrostatic pressure that forces fluid from the vascular space into the peritoneal cavity, compounded by hypoalbuminemia reducing oncotic pressure. Splenomegaly arises from congestive enlargement due to portal hypertension, leading to increased blood pooling and impaired splenic venous outflow. Both conditions frequently coexist in chronic liver diseases, where cirrhosis disrupts normal hepatic architecture and blood flow, driving these pathophysiological changes.
Clinical Presentation: Signs and Symptoms Comparison
Ascites presents clinically with abdominal distension, shifting dullness, and fluid wave due to excess fluid accumulation in the peritoneal cavity. Splenomegaly is characterized by palpable enlargement of the spleen, often accompanied by left upper quadrant discomfort, early satiety, or signs of underlying hematologic disorders. Both conditions may share symptoms such as abdominal discomfort and fatigue, but ascites primarily causes diffuse abdominal swelling, while splenomegaly involves localized enlargement detectable on physical examination.
Diagnostic Approaches for Ascites and Splenomegaly
Diagnostic approaches for ascites include physical examination techniques such as shifting dullness and fluid wave tests, along with imaging modalities like abdominal ultrasound, which provides sensitive detection of even small fluid volumes. Paracentesis is performed to analyze ascitic fluid, distinguishing between transudate and exudate causes and detecting infections or malignancies. Splenomegaly diagnosis relies on palpation and percussion during physical exams, with ultrasonography offering precise measurement of spleen size and CT or MRI scans aiding in assessing underlying etiologies such as hematologic disorders or portal hypertension.
Common Underlying Diseases and Risk Factors
Ascites commonly arises from liver cirrhosis, heart failure, or malignancies, with hepatitis B and C infections being significant risk factors. Splenomegaly frequently results from hematologic disorders such as lymphoma, leukemia, or portal hypertension associated with cirrhosis. Both conditions share chronic liver disease as a common underlying cause, but ascites primarily reflects fluid accumulation, while splenomegaly indicates splenic enlargement due to congestion or infiltration.
Complications Associated With Each Condition
Ascites can lead to complications such as spontaneous bacterial peritonitis, electrolyte imbalances, and respiratory distress due to increased abdominal pressure. Splenomegaly often results in hypersplenism, causing cytopenias like anemia, leukopenia, and thrombocytopenia, and increased risk of infections or bleeding. Both conditions commonly arise in liver cirrhosis but necessitate different management approaches to prevent severe complications.
Management and Treatment Options
Management of ascites primarily involves dietary sodium restriction, diuretics such as spironolactone and furosemide, and therapeutic paracentesis for large-volume fluid removal. Splenomegaly treatment targets the underlying cause, including managing portal hypertension with beta-blockers or considering splenectomy in cases of hypersplenism causing cytopenias. Both conditions require monitoring for complications, with ascites demanding vigilance for spontaneous bacterial peritonitis and splenomegaly requiring assessment for potential hematologic or infectious etiologies.
Prognosis and Long-Term Outcomes
Ascites often indicates advanced liver disease or malignancy, correlating with a poorer prognosis due to complications like spontaneous bacterial peritonitis and renal failure. Splenomegaly, commonly associated with portal hypertension or hematologic disorders, has variable long-term outcomes depending on the underlying cause and the development of hypersplenism or splenic infarction. Early diagnosis and management of ascites and splenomegaly significantly influence survival rates and quality of life in affected patients.
Ascites Infographic