Chorea is a neurological disorder characterized by involuntary, rapid, and irregular movements that can affect various body parts, causing challenges in coordination and balance. This condition often results from genetic factors, autoimmune diseases, or as a side effect of certain medications, impacting daily activities and quality of life. Explore the rest of the article to understand more about chorea's causes, symptoms, and treatment options to better manage your health.
Table of Comparison
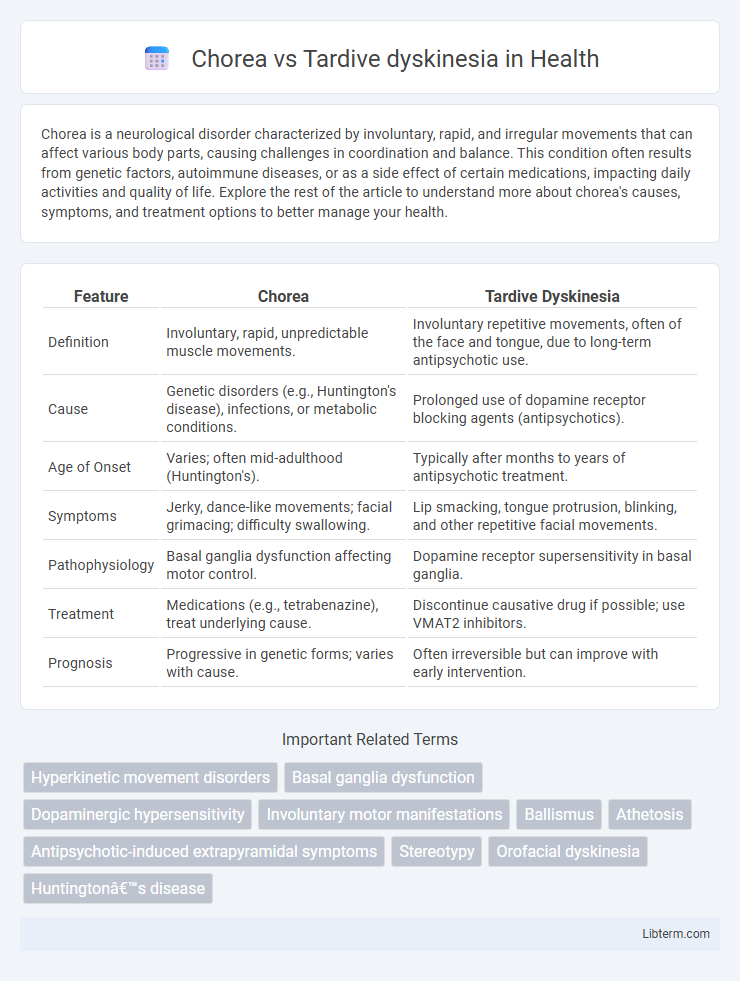
| Feature | Chorea | Tardive Dyskinesia |
|---|---|---|
| Definition | Involuntary, rapid, unpredictable muscle movements. | Involuntary repetitive movements, often of the face and tongue, due to long-term antipsychotic use. |
| Cause | Genetic disorders (e.g., Huntington's disease), infections, or metabolic conditions. | Prolonged use of dopamine receptor blocking agents (antipsychotics). |
| Age of Onset | Varies; often mid-adulthood (Huntington's). | Typically after months to years of antipsychotic treatment. |
| Symptoms | Jerky, dance-like movements; facial grimacing; difficulty swallowing. | Lip smacking, tongue protrusion, blinking, and other repetitive facial movements. |
| Pathophysiology | Basal ganglia dysfunction affecting motor control. | Dopamine receptor supersensitivity in basal ganglia. |
| Treatment | Medications (e.g., tetrabenazine), treat underlying cause. | Discontinue causative drug if possible; use VMAT2 inhibitors. |
| Prognosis | Progressive in genetic forms; varies with cause. | Often irreversible but can improve with early intervention. |
Introduction to Chorea and Tardive Dyskinesia
Chorea is a neurological disorder characterized by involuntary, rapid, irregular jerking movements primarily affecting the face, hands, and feet. Tardive dyskinesia is a medication-induced movement disorder marked by repetitive, involuntary movements, often involving the tongue, lips, and jaw, commonly resulting from long-term use of antipsychotic drugs. Both conditions arise from basal ganglia dysfunction but differ in etiology, symptom presentation, and treatment approaches.
Defining Chorea: Key Features and Causes
Chorea is characterized by rapid, involuntary, irregular movements primarily affecting the limbs, face, and trunk, often seen in conditions like Huntington's disease and rheumatic fever. Unlike tardive dyskinesia, which results from long-term use of dopamine receptor-blocking agents, chorea is linked to genetic mutations, autoimmune disorders, or metabolic abnormalities. Key features include unpredictable muscle twitches and impaired coordination, with causes rooted in basal ganglia dysfunction and neurochemical imbalances.
Understanding Tardive Dyskinesia: Overview and Origins
Tardive dyskinesia is a neurological disorder characterized by involuntary, repetitive movements, frequently caused by long-term use of dopamine receptor-blocking medications such as antipsychotics. Unlike chorea, which presents as rapid, unpredictable, and jerky movements often linked to neurological conditions like Huntington's disease, tardive dyskinesia manifests as slow, writhing motions predominantly affecting the face, tongue, and limbs. Understanding tardive dyskinesia involves recognizing its medication-induced origins and differentiating its persistent motor symptoms from the typically transient and purposeless movements of chorea.
Distinguishing Clinical Manifestations
Chorea is characterized by rapid, involuntary, irregular, and unpredictable movements often affecting the face, hands, and feet, commonly seen in Huntington's disease and rheumatic fever. Tardive dyskinesia presents with slow, repetitive, and stereotyped movements, primarily involving the orofacial region such as grimacing, tongue protrusion, and lip smacking, typically resulting from long-term use of dopamine receptor antagonists. The key clinical distinction lies in chorea's fluid, fleeting movements compared to the more persistent, patterned, and medication-induced nature of tardive dyskinesia.
Underlying Pathophysiology Differences
Chorea results from dysfunction in the basal ganglia, particularly involving imbalances in dopamine, gamma-aminobutyric acid (GABA), and acetylcholine neurotransmission within the striatum. Tardive dyskinesia primarily arises from prolonged dopamine receptor blockade leading to dopamine receptor supersensitivity and neuroplastic changes in the basal ganglia's nigrostriatal pathway. These distinct pathophysiological mechanisms differentiate chorea, often linked to genetic, autoimmune, or metabolic causes, from tardive dyskinesia, which is typically a consequence of long-term antipsychotic medication use.
Common Causes and Risk Factors
Chorea is often caused by genetic disorders such as Huntington's disease or autoimmune conditions like Sydenham's chorea, whereas tardive dyskinesia primarily results from long-term use of dopamine receptor-blocking agents, particularly antipsychotic medications. Risk factors for chorea include family history and acute infections, while tardive dyskinesia risk increases with age, cumulative exposure to neuroleptics, and underlying neurological disorders. Both conditions involve abnormal involuntary movements but originate from distinct pathophysiological mechanisms and etiologies.
Diagnostic Approaches and Criteria
Chorea is diagnosed through clinical evaluation emphasizing irregular, rapid, and unpredictable movements often linked to Huntington's disease or other neurodegenerative disorders, supported by genetic testing and neuroimaging. Tardive dyskinesia diagnosis relies on identification of repetitive, involuntary movements typically involving the face and mouth, emerging after prolonged use of dopamine receptor-blocking agents, confirmed by detailed medication history and exclusion of other movement disorders. Both conditions require comprehensive neurological examination and differentiation based on movement patterns, onset timing, and patient history for accurate diagnosis.
Impact on Quality of Life
Chorea causes rapid, involuntary movements that can disrupt daily activities and social interactions, often leading to emotional distress and decreased independence. Tardive dyskinesia involves repetitive, uncontrollable facial and limb movements that affect speech, eating, and self-esteem, resulting in significant psychological and functional impairment. Both conditions severely impact quality of life by limiting physical abilities and increasing isolation.
Treatment Strategies and Management
Treatment strategies for chorea often involve addressing the underlying cause, such as using dopamine-depleting agents like tetrabenazine or antipsychotics to reduce involuntary movements. Tardive dyskinesia management focuses on minimizing exposure to dopamine receptor-blocking agents and utilizing VMAT2 inhibitors such as valbenazine or deutetrabenazine to alleviate symptoms. Regular monitoring and individualized therapy adjustments are critical in both conditions to optimize functional outcomes and reduce adverse effects.
Prognosis and Long-Term Outcomes
Chorea often presents with unpredictable fluctuations and may improve or resolve depending on the underlying cause, while tardive dyskinesia (TD) typically results from prolonged neuroleptic use and tends to persist or worsen over time if exposure continues. Long-term outcomes for chorea vary widely, with some patients experiencing remission, whereas TD is usually considered irreversible, with only partial symptom control achievable through medication adjustments or neuromodulation. Early identification and management of causative factors significantly influence prognosis in both movement disorders, but tardive dyskinesia generally carries a more chronic and disabling course compared to chorea.
Chorea Infographic