Dystonia is a neurological movement disorder characterized by involuntary muscle contractions that cause repetitive movements or abnormal postures. Symptoms can range from mild to severe, affecting daily activities and overall quality of life. Discover how understanding dystonia can help you manage its challenges effectively in the rest of this article.
Table of Comparison
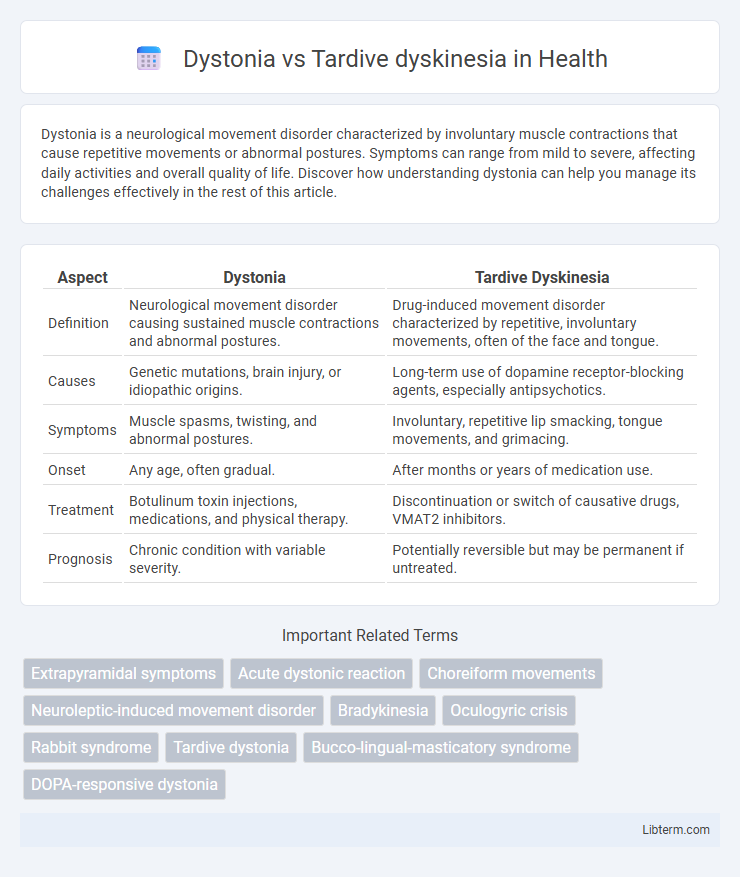
| Aspect | Dystonia | Tardive Dyskinesia |
|---|---|---|
| Definition | Neurological movement disorder causing sustained muscle contractions and abnormal postures. | Drug-induced movement disorder characterized by repetitive, involuntary movements, often of the face and tongue. |
| Causes | Genetic mutations, brain injury, or idiopathic origins. | Long-term use of dopamine receptor-blocking agents, especially antipsychotics. |
| Symptoms | Muscle spasms, twisting, and abnormal postures. | Involuntary, repetitive lip smacking, tongue movements, and grimacing. |
| Onset | Any age, often gradual. | After months or years of medication use. |
| Treatment | Botulinum toxin injections, medications, and physical therapy. | Discontinuation or switch of causative drugs, VMAT2 inhibitors. |
| Prognosis | Chronic condition with variable severity. | Potentially reversible but may be permanent if untreated. |
Introduction to Dystonia and Tardive Dyskinesia
Dystonia is a neurological movement disorder characterized by involuntary muscle contractions causing repetitive or twisting movements and abnormal postures, often linked to dysfunction in the basal ganglia. Tardive dyskinesia is a drug-induced condition, typically resulting from long-term use of antipsychotic medications, manifesting as repetitive, involuntary movements, particularly in the face, lips, and tongue. Both disorders involve abnormal motor control but differ in etiology, clinical presentation, and treatment approaches.
Defining Dystonia: Symptoms and Types
Dystonia is a neurological movement disorder characterized by involuntary muscle contractions causing repetitive twisting, abnormal postures, or spasms, often worsening with voluntary movement. Symptoms vary from focal dystonia affecting a specific body part, such as cervical dystonia impacting the neck, to generalized dystonia involving multiple muscle groups across the body. Unlike tardive dyskinesia, which primarily manifests as repetitive, involuntary movements due to long-term antipsychotic use, dystonia's distinct symptom profile includes sustained muscle contractions and abnormal posturing.
Understanding Tardive Dyskinesia: Key Characteristics
Tardive dyskinesia (TD) is a neurological disorder characterized by involuntary, repetitive movements, primarily affecting the face, tongue, and limbs, often resulting from long-term use of dopamine receptor-blocking agents like antipsychotics. Unlike dystonia, which involves sustained muscle contractions causing twisting and abnormal postures, TD typically presents with choreiform or athetoid motions that are more fluid and rapid. Early recognition of TD's symptoms is critical for preventing progression, as the condition can become irreversible if not promptly addressed.
Etiology: Causes of Dystonia vs Tardive Dyskinesia
Dystonia primarily arises from genetic mutations, brain injury, or abnormalities in basal ganglia function, often linked to neurotransmitter imbalances such as dopamine and acetylcholine. Tardive dyskinesia is a drug-induced movement disorder caused mainly by long-term use of dopamine receptor-blocking agents, especially antipsychotic medications. While dystonia involves intrinsic neurological dysfunction, tardive dyskinesia results from pharmacological receptor sensitization and neurochemical changes due to medication exposure.
Risk Factors and Affected Populations
Dystonia primarily affects individuals with a family history of the disorder or those exposed to certain medications, such as antipsychotics and dopamine receptor blockers, with risk increasing in younger adults and children. Tardive dyskinesia predominantly develops in older adults, especially those with prolonged use of antipsychotic drugs, and is more common among individuals with mood disorders or schizophrenia. Both conditions exhibit higher prevalence among females and populations with underlying neurological vulnerabilities.
Clinical Presentation: Differentiating Signs
Dystonia presents with sustained or intermittent muscle contractions causing abnormal postures or repetitive movements, often involving the neck, limbs, or face. Tardive dyskinesia is characterized by involuntary, repetitive, and irregular movements, primarily affecting the orofacial region with choreiform or athetoid features. Unlike dystonia's prolonged muscle spasms, tardive dyskinesia typically manifests as rapid, jerky motions linked to long-term antipsychotic use.
Diagnostic Approaches and Testing
Diagnostic approaches for dystonia primarily involve clinical evaluation of sustained muscle contractions and abnormal postures, supported by genetic testing and neuroimaging to identify underlying causes or rule out secondary dystonia. In contrast, tardive dyskinesia diagnosis relies on a thorough medication history, particularly prolonged use of antipsychotics, combined with observation of involuntary, repetitive movements and the Abnormal Involuntary Movement Scale (AIMS) for severity assessment. Both conditions may require electromyography (EMG) to differentiate muscle activity patterns, enhancing diagnostic accuracy.
Treatment Options for Dystonia
Dystonia treatment primarily involves medications such as anticholinergics, muscle relaxants, and botulinum toxin injections, which help reduce muscle contractions and spasms. Deep brain stimulation (DBS) is an advanced option for patients with severe or medication-resistant dystonia, offering significant symptom relief by targeting specific brain areas. Physical therapy and supportive care also play essential roles in managing dystonia symptoms and improving quality of life.
Management and Therapy for Tardive Dyskinesia
Management of tardive dyskinesia primarily involves discontinuation or dose reduction of offending antipsychotic medications when clinically feasible, alongside switching to atypical antipsychotics with lower risk profiles. Pharmacological therapies for tardive dyskinesia include VMAT2 inhibitors such as valbenazine and deutetrabenazine, which have demonstrated efficacy in reducing involuntary movements. Supportive treatments may involve botulinum toxin injections and physical therapy to improve motor function and quality of life in affected patients.
Prognosis and Quality of Life Considerations
Dystonia prognosis varies widely, with some patients experiencing progressive symptoms while others achieve symptom control through treatments like botulinum toxin or deep brain stimulation, significantly improving quality of life. Tardive dyskinesia often persists or worsens after antipsychotic discontinuation, with limited response to treatment, leading to chronic involuntary movements that can severely impact daily functioning and psychosocial well-being. Both conditions require early diagnosis and multidisciplinary management to optimize long-term outcomes and maintain patient quality of life.
Dystonia Infographic