Coccidioidomycosis, also known as valley fever, is a fungal infection caused by Coccidioides species found in soil of arid regions. Symptoms range from mild respiratory issues to severe complications, especially in immunocompromised individuals. Explore the rest of the article to understand how you can recognize, prevent, and manage this potentially serious disease.
Table of Comparison
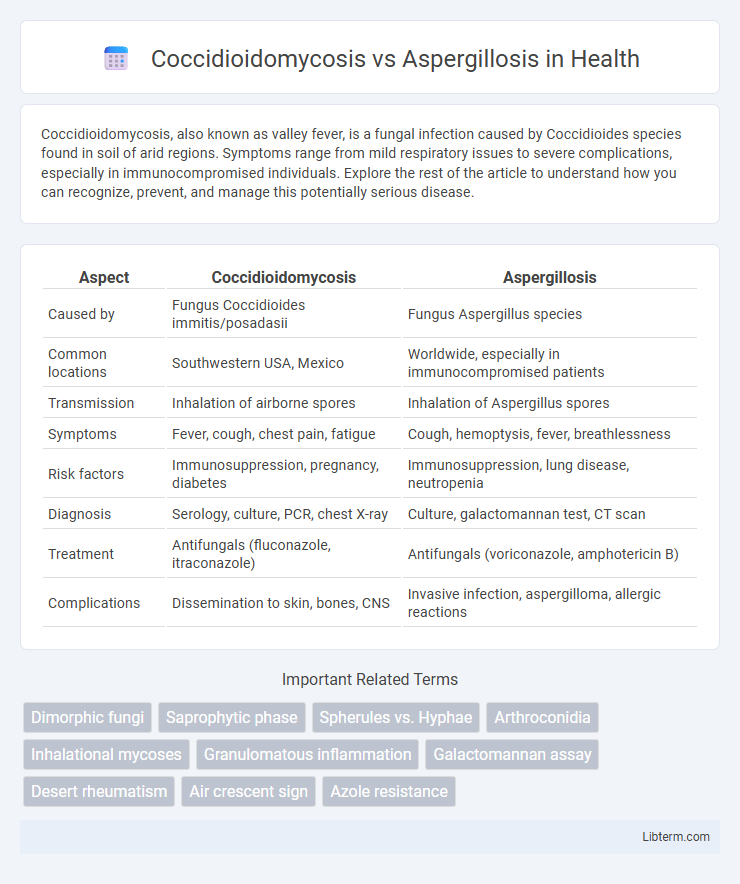
| Aspect | Coccidioidomycosis | Aspergillosis |
|---|---|---|
| Caused by | Fungus Coccidioides immitis/posadasii | Fungus Aspergillus species |
| Common locations | Southwestern USA, Mexico | Worldwide, especially in immunocompromised patients |
| Transmission | Inhalation of airborne spores | Inhalation of Aspergillus spores |
| Symptoms | Fever, cough, chest pain, fatigue | Cough, hemoptysis, fever, breathlessness |
| Risk factors | Immunosuppression, pregnancy, diabetes | Immunosuppression, lung disease, neutropenia |
| Diagnosis | Serology, culture, PCR, chest X-ray | Culture, galactomannan test, CT scan |
| Treatment | Antifungals (fluconazole, itraconazole) | Antifungals (voriconazole, amphotericin B) |
| Complications | Dissemination to skin, bones, CNS | Invasive infection, aspergilloma, allergic reactions |
Introduction to Coccidioidomycosis and Aspergillosis
Coccidioidomycosis, also known as Valley fever, is a fungal infection caused by Coccidioides species, primarily affecting the lungs and prevalent in arid regions of the southwestern United States and parts of Central and South America. Aspergillosis results from Aspergillus species, a common mold found worldwide, and primarily affects immunocompromised individuals through respiratory tract colonization or invasive disease. Both conditions present diagnostic challenges due to overlapping respiratory symptoms but differ in causative fungi, geographic distribution, and clinical manifestations.
Etiological Agents: Causative Fungi Compared
Coccidioidomycosis is caused by the dimorphic fungi Coccidioides immitis and Coccidioides posadasii, which thrive in arid soil environments primarily in the southwestern United States and parts of Central and South America. Aspergillosis results from inhaling spores of Aspergillus species, mainly Aspergillus fumigatus, a ubiquitous mold found in decaying organic matter and soil worldwide. Both infections involve inhalation of airborne spores but differ significantly in fungal morphology, geographic distribution, and pathogenic mechanisms.
Geographic Distribution and Epidemiology
Coccidioidomycosis, also known as Valley fever, predominantly affects arid regions of the southwestern United States, particularly Arizona and California, with endemic foci extending into parts of Mexico and Central and South America. Aspergillosis, caused by Aspergillus species, has a global distribution but is more common in immunocompromised individuals and airborne spore exposure settings, including damp or decaying vegetation environments worldwide. Epidemiologically, coccidioidomycosis incidence can spike following dust storms and earthquakes, while aspergillosis incidence rises in hospital environments with high risk patients and agricultural workers exposed to fungal spores.
Modes of Transmission
Coccidioidomycosis is primarily transmitted through inhalation of airborne spores from disturbed soil in arid regions, notably the southwestern United States. Aspergillosis results from inhaling ubiquitous Aspergillus spores found in decaying organic matter, soil, and indoor environments with mold contamination. Both infections initiate in the respiratory system after spore inhalation but differ significantly in environmental reservoirs and geographic distribution.
Clinical Manifestations and Symptoms
Coccidioidomycosis primarily presents with flu-like symptoms such as fever, cough, chest pain, and fatigue, often accompanied by erythema nodosum or erythema multiforme in disseminated cases. Aspergillosis commonly manifests with respiratory symptoms including wheezing, hemoptysis, and pleuritic chest pain, frequently occurring in immunocompromised patients or those with underlying lung disease. Both infections can lead to severe pulmonary complications, but aspergillosis often involves invasive tissue damage and allergic bronchopulmonary responses.
Diagnostic Approaches and Laboratory Findings
Coccidioidomycosis diagnosis primarily relies on serologic tests detecting IgM and IgG antibodies, complemented by fungal culture and histopathology revealing spherules with endospores, whereas Aspergillosis diagnosis involves culture and histopathology demonstrating septate hyphae with acute angle branching, alongside galactomannan antigen testing and beta-D-glucan assays. PCR-based methods serve as valuable tools for both infections, enhancing sensitivity in clinical specimens. Laboratory findings for coccidioidomycosis often include eosinophilia and elevated complement fixation titers, while aspergillosis frequently presents with elevated serum galactomannan and imaging showing characteristic lung nodules or cavitations.
Radiological Differences
Coccidioidomycosis typically presents with nodules, cavities, or diffuse pulmonary infiltrates on chest X-rays, often affecting the upper lobes with potential calcified granulomas visible on CT scans. Aspergillosis demonstrates characteristic radiological features such as the "fungus ball" (aspergilloma) within preexisting lung cavities or the halo sign and air crescent sign on CT imaging, especially in invasive forms. Radiological differentiation is aided by the presence of cavitary lesions with fungal balls in aspergillosis versus widespread nodular patterns and calcifications predominantly seen in coccidioidomycosis.
Treatment Strategies and Antifungal Therapies
Coccidioidomycosis treatment primarily involves antifungal agents such as fluconazole or itraconazole, with amphotericin B reserved for severe or disseminated cases. Aspergillosis management depends on disease form, using voriconazole as first-line therapy, while amphotericin B or echinocandins serve as alternatives for invasive infections. Both infections require tailored antifungal regimens based on patient immune status and severity, emphasizing early diagnosis to optimize therapeutic outcomes.
Prognosis and Complication Risks
Coccidioidomycosis prognosis varies based on disease severity, with uncomplicated cases resolving spontaneously but severe or disseminated forms causing chronic lung disease or meningitis. Aspergillosis prognosis depends on infection type; invasive aspergillosis often has a high mortality rate in immunocompromised patients, while allergic or chronic forms show better outcomes with management. Both infections carry risks of significant complications such as respiratory failure, dissemination, and secondary bacterial infections, necessitating prompt diagnosis and tailored antifungal therapy.
Prevention and Public Health Implications
Preventing Coccidioidomycosis involves controlling exposure to Coccidioides spores primarily found in arid soil of the southwestern United States, emphasizing dust control and protective masks for high-risk populations. Aspergillosis prevention focuses on minimizing contact with Aspergillus spores present in decaying organic matter, especially in hospital settings, by employing HEPA filtration and sterilization protocols. Both diseases pose significant public health challenges due to their respiratory infection potential, requiring targeted surveillance, education, and robust environmental control measures to reduce incidence and mitigate severe outcomes in immunocompromised individuals.
Coccidioidomycosis Infographic