Sarcoidosis is an inflammatory disease characterized by the formation of tiny clumps of inflammatory cells called granulomas in various organs, commonly affecting the lungs and lymph nodes. Its symptoms range from mild to severe, including persistent cough, fatigue, and skin lesions, often making diagnosis challenging. Explore the rest of the article to understand the causes, symptoms, and treatment options for your optimal health management.
Table of Comparison
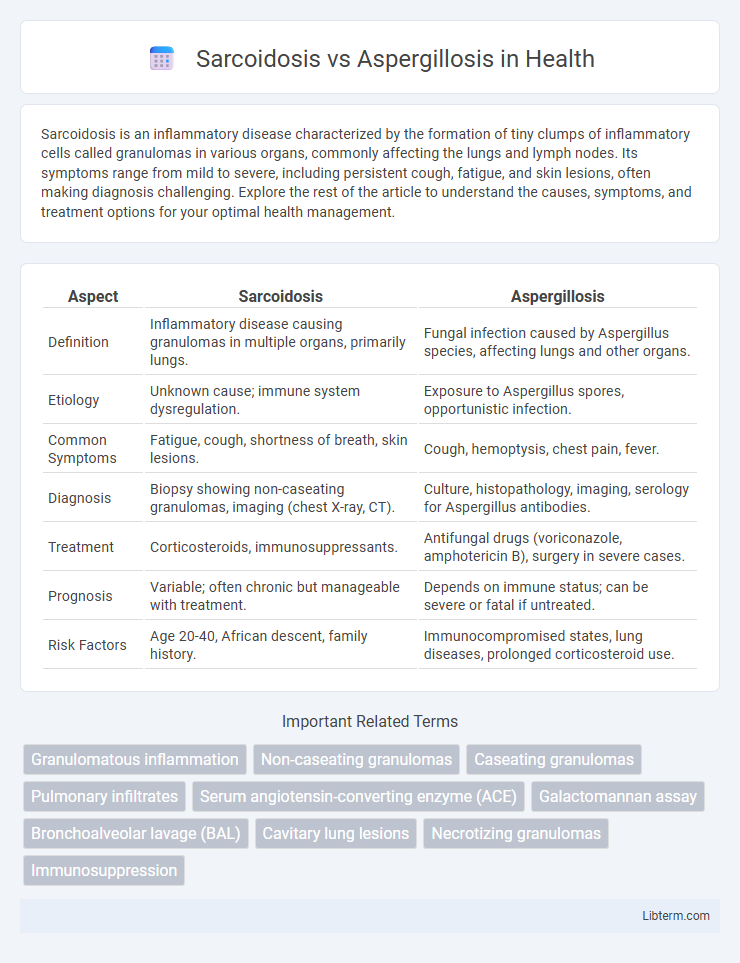
| Aspect | Sarcoidosis | Aspergillosis |
|---|---|---|
| Definition | Inflammatory disease causing granulomas in multiple organs, primarily lungs. | Fungal infection caused by Aspergillus species, affecting lungs and other organs. |
| Etiology | Unknown cause; immune system dysregulation. | Exposure to Aspergillus spores, opportunistic infection. |
| Common Symptoms | Fatigue, cough, shortness of breath, skin lesions. | Cough, hemoptysis, chest pain, fever. |
| Diagnosis | Biopsy showing non-caseating granulomas, imaging (chest X-ray, CT). | Culture, histopathology, imaging, serology for Aspergillus antibodies. |
| Treatment | Corticosteroids, immunosuppressants. | Antifungal drugs (voriconazole, amphotericin B), surgery in severe cases. |
| Prognosis | Variable; often chronic but manageable with treatment. | Depends on immune status; can be severe or fatal if untreated. |
| Risk Factors | Age 20-40, African descent, family history. | Immunocompromised states, lung diseases, prolonged corticosteroid use. |
Introduction to Sarcoidosis and Aspergillosis
Sarcoidosis is a systemic inflammatory disease characterized by the formation of non-caseating granulomas, predominantly affecting the lungs and lymphatic system, with unclear etiology linked to immune dysregulation. Aspergillosis is an infectious condition caused by Aspergillus species, primarily affecting immunocompromised individuals and manifesting in forms such as invasive pulmonary aspergillosis, allergic bronchopulmonary aspergillosis (ABPA), and aspergilloma. Both diseases impact respiratory health but differ fundamentally in pathogenesis, diagnostic criteria, and therapeutic approaches.
Etiology: Causes and Risk Factors
Sarcoidosis is primarily caused by an abnormal immune response leading to granuloma formation, with genetic predisposition and environmental factors such as exposure to certain dusts or infections being significant risk contributors. Aspergillosis results from infection by Aspergillus fungi, predominantly affecting individuals with weakened immune systems, underlying lung diseases, or those exposed to high levels of fungal spores in environments like decaying vegetation or construction sites. Both conditions involve immune system interactions, but sarcoidosis is an autoimmune disorder while aspergillosis is an opportunistic fungal infection.
Pathophysiology: How Each Disease Develops
Sarcoidosis develops through an abnormal immune response characterized by the formation of non-caseating granulomas mainly in the lungs and lymph nodes, driven by T-helper cell activation and macrophage accumulation. Aspergillosis occurs due to inhalation of Aspergillus spores, leading to colonization and invasion, especially in immunocompromised individuals, causing tissue necrosis and inflammation. The key difference lies in sarcoidosis being an autoimmune granulomatous disease, whereas aspergillosis results from fungal infection and subsequent immune reaction.
Clinical Manifestations: Signs and Symptoms
Sarcoidosis commonly presents with bilateral hilar lymphadenopathy, persistent dry cough, dyspnea, and erythema nodosum, whereas aspergillosis manifests with symptoms ranging from allergic bronchopulmonary reactions like wheezing and mucus production to invasive pulmonary disease characterized by fever, chest pain, and hemoptysis. Sarcoidosis often involves systemic signs such as fatigue, weight loss, and night sweats, while aspergillosis symptoms vary by type, with chronic forms causing progressive lung damage and aspergilloma leading to recurrent coughing and blood-streaked sputum. Both conditions may show respiratory distress, but the presence of granulomas in sarcoidosis contrasts with fungal hyphae invasion in aspergillosis identifiable through imaging and biopsy.
Diagnostic Challenges: Differentiating Sarcoidosis from Aspergillosis
Sarcoidosis and aspergillosis present overlapping clinical and radiographic features, complicating accurate diagnosis. Sarcoidosis often exhibits non-caseating granulomas on biopsy, while aspergillosis shows fungal hyphae and necrosis, but invasive fungal elements may be missed in limited samples. Advanced imaging, serum biomarkers such as angiotensin-converting enzyme (ACE) for sarcoidosis and galactomannan antigen for aspergillosis, alongside molecular diagnostics, are critical to distinguishing these conditions and guiding appropriate therapy.
Imaging Findings: Radiological Clues
Sarcoidosis typically presents on chest X-rays and CT scans with bilateral hilar lymphadenopathy, perilymphatic nodules, and upper lobe predominant pulmonary infiltrates, often forming a characteristic "lambda sign" on gallium scans. In contrast, aspergillosis imaging often reveals cavitary lesions, fungal balls (aspergillomas) within pre-existing cavities, and halo signs or air crescent signs on CT, indicative of invasive or allergic forms. Differentiating these conditions relies heavily on identifying patterns such as lymphadenopathy and nodular distributions in sarcoidosis versus cavitation and fungal masses in aspergillosis.
Laboratory and Histopathological Features
Sarcoidosis is characterized by non-caseating granulomas in histopathology, often with elevated serum angiotensin-converting enzyme (ACE) levels and hypercalcemia, while Aspergillosis shows variable histological presence of septate hyphae with acute angle branching and positive galactomannan antigen tests in laboratory assays. Sarcoidosis typically lacks infectious organisms on special staining, contrasting with Aspergillosis where Gomori methenamine silver (GMS) or periodic acid-Schiff (PAS) stains highlight fungal elements. Both conditions may show granulomatous inflammation, but Aspergillosis demonstrates tissue invasion and necrosis, aiding differentiation through combined histopathological evaluation and fungal biomarkers.
Treatment Approaches
Treatment approaches for sarcoidosis primarily involve corticosteroids such as prednisone to reduce inflammation and immune system activity, with immunosuppressive agents like methotrexate or azathioprine used in steroid-resistant cases. Aspergillosis treatment relies heavily on antifungal medications such as voriconazole or amphotericin B to combat Aspergillus infections, with surgical intervention considered for severe or invasive cases. The choice of therapy for sarcoidosis versus aspergillosis depends on the underlying etiology, with immunosuppression critical in sarcoidosis and antifungal eradication essential in aspergillosis management.
Prognosis and Complications
Sarcoidosis generally has a favorable prognosis with spontaneous remission in many cases, but chronic disease can lead to pulmonary fibrosis and organ dysfunction. Aspergillosis, particularly invasive forms, carries a poorer prognosis due to aggressive tissue invasion, often causing severe complications like necrotizing pneumonia and systemic dissemination. Both conditions risk chronic respiratory impairment, yet aspergillosis requires prompt antifungal treatment to reduce morbidity and mortality.
Key Differences and Summary Table
Sarcoidosis is a multisystem inflammatory disease characterized by non-caseating granulomas, primarily affecting the lungs and lymph nodes, whereas Aspergillosis is a fungal infection caused by Aspergillus species, predominantly impacting immunocompromised individuals. Sarcoidosis presents with bilateral hilar lymphadenopathy and hypercalcemia, while Aspergillosis manifests with lung cavitations, allergic bronchopulmonary symptoms, or invasive fungal growth. Key differences include etiology, immune response involvement, and diagnostic markers such as serum angiotensin-converting enzyme levels for Sarcoidosis and galactomannan antigen detection for Aspergillosis.
Sarcoidosis Infographic