Hypochromia refers to a condition where red blood cells have less color than normal due to reduced hemoglobin content, often indicating underlying anemia or iron deficiency. This alteration impacts the cells' oxygen-carrying capacity, leading to fatigue and weakness. Discover how recognizing hypochromia can help you understand your blood health more comprehensively in the rest of the article.
Table of Comparison
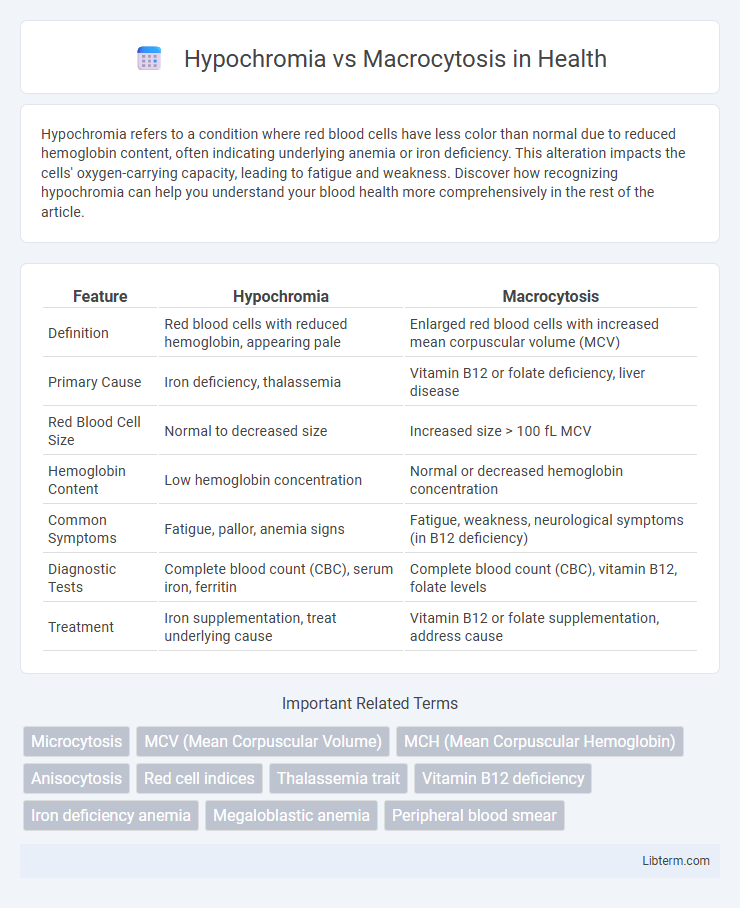
| Feature | Hypochromia | Macrocytosis |
|---|---|---|
| Definition | Red blood cells with reduced hemoglobin, appearing pale | Enlarged red blood cells with increased mean corpuscular volume (MCV) |
| Primary Cause | Iron deficiency, thalassemia | Vitamin B12 or folate deficiency, liver disease |
| Red Blood Cell Size | Normal to decreased size | Increased size > 100 fL MCV |
| Hemoglobin Content | Low hemoglobin concentration | Normal or decreased hemoglobin concentration |
| Common Symptoms | Fatigue, pallor, anemia signs | Fatigue, weakness, neurological symptoms (in B12 deficiency) |
| Diagnostic Tests | Complete blood count (CBC), serum iron, ferritin | Complete blood count (CBC), vitamin B12, folate levels |
| Treatment | Iron supplementation, treat underlying cause | Vitamin B12 or folate supplementation, address cause |
Understanding Hypochromia: Definition and Causes
Hypochromia is characterized by red blood cells that have reduced hemoglobin content, resulting in paler-than-normal cells often seen in iron deficiency anemia and thalassemia. The condition highlights impaired hemoglobin synthesis, which can be linked to nutritional deficiencies, chronic inflammation, or genetic disorders affecting globin production. Differentiating hypochromia from macrocytosis, where red blood cells are abnormally large, is crucial for accurate diagnosis and targeted treatment in various anemias.
What Is Macrocytosis? Key Features and Etiology
Macrocytosis is characterized by the presence of abnormally large red blood cells, often identified through an increased mean corpuscular volume (MCV) above 100 femtoliters. Key features include impaired DNA synthesis resulting in delayed nuclear maturation, which leads to enlarged erythrocytes typically observed in peripheral blood smears. Etiology commonly involves vitamin B12 or folate deficiency, liver disease, hypothyroidism, and certain medications such as hydroxyurea or methotrexate.
Hypochromia vs Macrocytosis: Key Differences
Hypochromia is characterized by red blood cells with reduced hemoglobin content, resulting in paler cells and is commonly associated with iron deficiency anemia. Macrocytosis involves enlarged red blood cells, often linked to vitamin B12 or folate deficiency and various bone marrow disorders. The key differences lie in cell size and hemoglobin concentration, where hypochromia has normal to small cell size with decreased color intensity, while macrocytosis features increased cell size with typically normal hemoglobin content.
Pathophysiology of Hypochromia
Hypochromia is characterized by decreased hemoglobin concentration in red blood cells, often resulting from impaired hemoglobin synthesis as seen in iron deficiency anemia. The pathophysiology involves insufficient iron supply, leading to reduced incorporation of heme into erythrocytes and producing pale (hypochromic) cells with decreased oxygen-carrying capacity. In contrast, macrocytosis reflects enlarged red blood cells due to impaired DNA synthesis, commonly caused by vitamin B12 or folate deficiency, affecting cell division rather than hemoglobin content.
Pathophysiology of Macrocytosis
Macrocytosis is characterized by the presence of abnormally large red blood cells, primarily caused by impaired DNA synthesis leading to delayed nuclear maturation and continued cytoplasmic growth. This disruption is often linked to deficiencies in vitamin B12 or folate, which are crucial cofactors in nucleotide production and cell division. In contrast to hypochromia, which involves decreased hemoglobin content, macrocytosis reflects altered erythropoiesis due to defective cell cycle progression and ineffective erythropoiesis.
Clinical Manifestations: Signs and Symptoms
Hypochromia typically presents with signs of anemia such as pallor, fatigue, and weakness due to reduced hemoglobin content in red blood cells, often seen in iron deficiency anemia. Macrocytosis manifests with symptoms related to vitamin B12 or folate deficiency, including glossitis, neuropathy, and megaloblastic anemia features, characterized by enlarged red blood cells. Both conditions exhibit distinct blood smear findings critical for differential diagnosis, with hypochromia showing hypochromic, microcytic cells and macrocytosis showing large, oval macrocytes.
Diagnostic Approaches for Hypochromia and Macrocytosis
Diagnostic approaches for hypochromia primarily include complete blood count (CBC) analysis revealing decreased mean corpuscular hemoglobin (MCH) and serum iron studies to identify iron deficiency anemia. Macrocytosis diagnosis involves CBC showing elevated mean corpuscular volume (MCV), peripheral blood smear examination for hypersegmented neutrophils, and assessment of vitamin B12 and folate levels to detect megaloblastic anemia. Bone marrow biopsy may be warranted in ambiguous cases to further differentiate underlying hematologic disorders.
Common Diseases Associated with Hypochromia and Macrocytosis
Hypochromia is commonly associated with iron-deficiency anemia, thalassemia, and chronic disease anemia, characterized by red blood cells with reduced hemoglobin content. Macrocytosis frequently appears in megaloblastic anemia due to vitamin B12 or folate deficiency, as well as in liver disease and hypothyroidism, reflecting enlarged red blood cells. Both conditions serve as important hematologic indicators for differentiating underlying pathological causes in clinical diagnostics.
Treatment Strategies: Hypochromia vs Macrocytosis
Treatment strategies for hypochromia typically involve addressing underlying iron deficiency through oral or intravenous iron supplementation and dietary modifications to restore normal hemoglobin synthesis. Macrocytosis management centers on correcting causes such as vitamin B12 or folate deficiency via targeted supplementation and monitoring for underlying conditions like bone marrow disorders. Both conditions require tailored approaches guided by hematologic evaluations and response to therapy to optimize patient outcomes.
Prognosis and Preventive Measures
Hypochromia, characterized by reduced hemoglobin content in red blood cells, often signals iron deficiency anemia, with a prognosis that improves significantly upon timely iron supplementation and dietary adjustments rich in bioavailable iron. Macrocytosis, marked by enlarged red blood cells, usually indicates vitamin B12 or folate deficiency and carries a variable prognosis depending on the underlying cause, ranging from reversible with proper vitamin replacement to complications if linked to bone marrow disorders. Preventive measures for hypochromia emphasize maintaining adequate iron intake and addressing chronic blood loss, while preventing macrocytosis involves ensuring sufficient vitamin B12 and folate through diet or supplementation and monitoring at-risk populations such as those with malabsorption syndromes or alcohol use.
Hypochromia Infographic