Akathisia is a movement disorder characterized by an uncontrollable urge to move, often accompanied by feelings of restlessness and anxiety. It commonly occurs as a side effect of certain medications, particularly antipsychotics and antidepressants, making early recognition crucial for effective management. Explore this article to understand the symptoms, causes, and treatment options for akathisia to improve your quality of life.
Table of Comparison
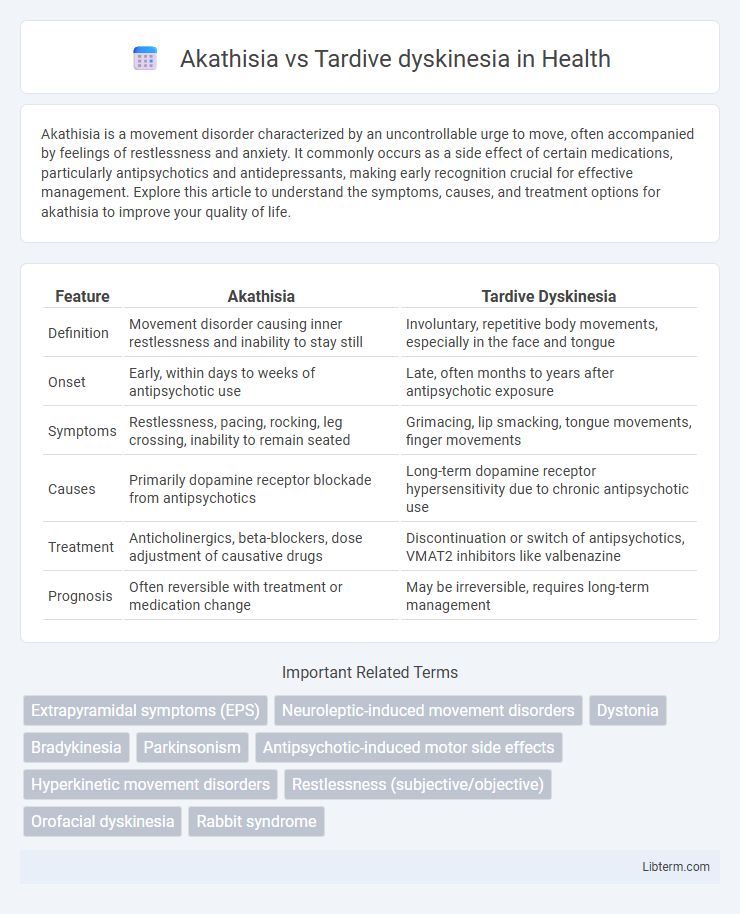
| Feature | Akathisia | Tardive Dyskinesia |
|---|---|---|
| Definition | Movement disorder causing inner restlessness and inability to stay still | Involuntary, repetitive body movements, especially in the face and tongue |
| Onset | Early, within days to weeks of antipsychotic use | Late, often months to years after antipsychotic exposure |
| Symptoms | Restlessness, pacing, rocking, leg crossing, inability to remain seated | Grimacing, lip smacking, tongue movements, finger movements |
| Causes | Primarily dopamine receptor blockade from antipsychotics | Long-term dopamine receptor hypersensitivity due to chronic antipsychotic use |
| Treatment | Anticholinergics, beta-blockers, dose adjustment of causative drugs | Discontinuation or switch of antipsychotics, VMAT2 inhibitors like valbenazine |
| Prognosis | Often reversible with treatment or medication change | May be irreversible, requires long-term management |
Introduction to Akathisia and Tardive Dyskinesia
Akathisia is a movement disorder characterized by an inner sense of restlessness and an uncontrollable need to move, often manifesting as pacing or fidgeting, commonly associated with antipsychotic medication use. Tardive dyskinesia involves repetitive, involuntary movements such as grimacing or tongue protrusion, typically emerging after prolonged exposure to dopamine receptor-blocking agents. Both conditions are classified as extrapyramidal side effects but differ in onset, symptom presentation, and underlying pathophysiology.
Defining Akathisia: Symptoms and Characteristics
Akathisia is a movement disorder characterized by an inner sense of restlessness and an uncontrollable urge to move, often resulting in repetitive motions such as pacing or leg crossing. Symptoms include constant fidgeting, rocking while standing or sitting, and an intense feeling of unease, typically emerging within days to weeks of antipsychotic medication use. Unlike tardive dyskinesia, which manifests as involuntary, slow, writhing movements primarily of the face and tongue, akathisia primarily affects the entire body and is driven by psychological discomfort combined with motor restlessness.
Understanding Tardive Dyskinesia: Signs and Manifestations
Tardive dyskinesia is characterized by involuntary, repetitive movements, often affecting the face, tongue, and limbs, resulting from long-term use of antipsychotic medications. Key signs include grimacing, lip smacking, and rapid blinking, which distinguish it from akathisia's motor restlessness and inner agitation. Early recognition of tardive dyskinesia symptoms is crucial for managing potential neurological damage and adjusting treatment plans effectively.
Key Differences Between Akathisia and Tardive Dyskinesia
Akathisia is characterized by an inner restlessness and an uncontrollable urge to move, often manifesting as pacing or fidgeting, whereas tardive dyskinesia involves repetitive, involuntary movements such as grimacing, lip smacking, or tongue protrusion. Akathisia symptoms typically appear shortly after starting or increasing antipsychotic medications, while tardive dyskinesia develops after long-term exposure, often months or years later. Management strategies differ significantly; akathisia may respond to dose reduction or beta-blockers, whereas tardive dyskinesia often requires specialized treatments like VMAT2 inhibitors.
Causes and Risk Factors of Akathisia
Akathisia primarily results from dopamine receptor blockade caused by antipsychotic medications, especially first-generation antipsychotics like haloperidol, and can also be triggered by certain antidepressants and antiemetics. Risk factors for Akathisia include higher doses of antipsychotics, rapid dose escalation, female gender, older age, and a history of movement disorders. Unlike Tardive dyskinesia, which arises after long-term dopamine receptor blockade leading to receptor supersensitivity, Akathisia develops rapidly and is often reversible with dose adjustment or medication changes.
Causes and Triggers of Tardive Dyskinesia
Tardive dyskinesia is primarily caused by long-term use of dopamine receptor-blocking agents, especially antipsychotic medications such as haloperidol and chlorpromazine. Chronic exposure to these drugs leads to dopamine receptor hypersensitivity and neurochemical imbalances in the basal ganglia, triggering involuntary, repetitive movements characteristic of the disorder. Risk factors include older age, diabetes, duration and dosage of antipsychotic treatment, and genetic predisposition.
Diagnosis: Differentiating Akathisia from Tardive Dyskinesia
Diagnosing akathisia involves identifying subjective feelings of inner restlessness and observable repetitive movements such as pacing or leg rocking, often emerging shortly after starting or increasing antipsychotic medications. Tardive dyskinesia is characterized by involuntary, repetitive movements, primarily of the face and tongue, developing after long-term use of dopamine receptor-blocking agents, distinguishable through clinical history and movement patterns. Clinicians rely on detailed patient history, temporal onset, and specific motor symptoms to differentiate between akathisia's constant restlessness and tardive dyskinesia's dyskinetic movements for accurate diagnosis and appropriate management.
Treatment Approaches for Akathisia
Treatment approaches for akathisia primarily involve reducing or discontinuing the causative antipsychotic medication, switching to a lower-risk drug such as quetiapine or clozapine, and administering beta-blockers like propranolol to alleviate restlessness. Benzodiazepines, such as lorazepam, and anticholinergic agents like benztropine are also commonly employed to manage symptoms. Early recognition and intervention are critical to prevent progression into more severe movement disorders, distinguishing akathisia management from tardive dyskinesia strategies that often require different pharmacological treatments such as VMAT2 inhibitors.
Management and Therapy for Tardive Dyskinesia
Management of Tardive Dyskinesia primarily involves cessation or reduction of the offending antipsychotic medication when feasible, alongside the introduction of FDA-approved treatments such as valbenazine or deutetrabenazine, which are vesicular monoamine transporter 2 (VMAT2) inhibitors shown to reduce involuntary movements. Supportive therapies including physical and occupational therapy can help improve functional abilities and quality of life for affected patients. Regular monitoring and early detection of symptoms are essential to prevent progression and optimize therapeutic outcomes in individuals with Tardive Dyskinesia.
Prevention Strategies and Prognosis for Both Conditions
Effective prevention strategies for akathisia include careful dose titration and selection of antipsychotic medications with lower extrapyramidal side effect profiles, while tardive dyskinesia prevention emphasizes minimizing long-term use of dopamine receptor blockers and regular monitoring for early symptoms. Prognosis for akathisia typically improves with prompt medication adjustments or addition of beta-blockers, whereas tardive dyskinesia may persist or worsen despite intervention, making early detection and prevention critical. Both conditions benefit from individualized treatment plans and ongoing neurological assessments to mitigate severity and improve patient quality of life.
Akathisia Infographic