Carboprost is a synthetic prostaglandin used primarily to induce labor and control postpartum hemorrhage by stimulating uterine contractions. Its effective role in managing obstetric complications makes it a critical medication in maternal healthcare. Explore the article to learn more about Carboprost's uses, dosage, and potential side effects to ensure its safe application for your medical needs.
Table of Comparison
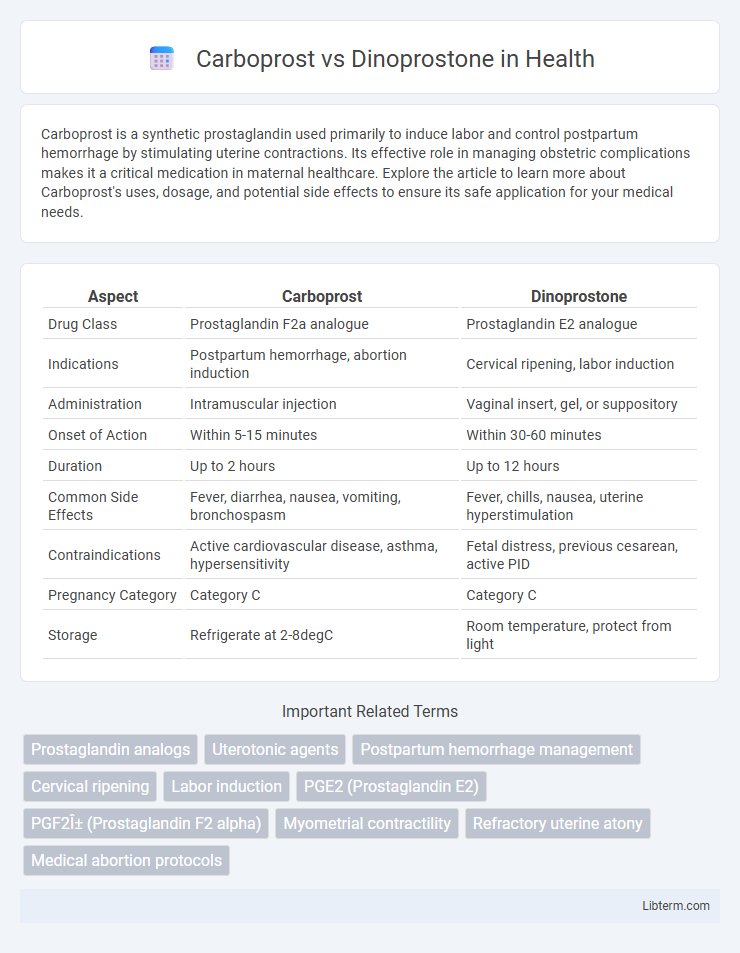
| Aspect | Carboprost | Dinoprostone |
|---|---|---|
| Drug Class | Prostaglandin F2a analogue | Prostaglandin E2 analogue |
| Indications | Postpartum hemorrhage, abortion induction | Cervical ripening, labor induction |
| Administration | Intramuscular injection | Vaginal insert, gel, or suppository |
| Onset of Action | Within 5-15 minutes | Within 30-60 minutes |
| Duration | Up to 2 hours | Up to 12 hours |
| Common Side Effects | Fever, diarrhea, nausea, vomiting, bronchospasm | Fever, chills, nausea, uterine hyperstimulation |
| Contraindications | Active cardiovascular disease, asthma, hypersensitivity | Fetal distress, previous cesarean, active PID |
| Pregnancy Category | Category C | Category C |
| Storage | Refrigerate at 2-8degC | Room temperature, protect from light |
Introduction to Carboprost and Dinoprostone
Carboprost is a synthetic prostaglandin analogue primarily used to induce labor and control postpartum hemorrhage by stimulating uterine contractions. Dinoprostone, also known as prostaglandin E2, facilitates cervical ripening and labor induction by promoting uterine muscle relaxation followed by contraction. Both medications play critical roles in obstetrics, with distinct pharmacological profiles that influence their clinical applications and dosing regimens.
Mechanisms of Action
Carboprost acts as a synthetic prostaglandin F2 alpha analog that induces strong uterine contractions by binding to prostaglandin F receptors, promoting calcium release in smooth muscle cells. Dinoprostone, a naturally occurring prostaglandin E2 analog, facilitates cervical ripening and stimulates uterine contractions through activation of prostaglandin E receptors, increasing intracellular cyclic AMP and calcium levels. These distinct receptor targets result in varied efficacy and side effect profiles in labor induction and postpartum hemorrhage management.
Clinical Indications
Carboprost is primarily indicated for the treatment of postpartum hemorrhage due to uterine atony when conventional methods fail, while Dinoprostone is mainly used for cervical ripening and labor induction in pregnant women at term. Carboprost acts as a potent uterotonic agent by stimulating strong uterine contractions, whereas Dinoprostone, a prostaglandin E2 analog, facilitates cervical softening and dilation to promote labor progression. Both drugs play essential roles in obstetric management, tailored to specific clinical scenarios involving labor initiation and control of bleeding post-delivery.
Efficacy Comparison
Carboprost demonstrates higher efficacy in controlling postpartum hemorrhage compared to Dinoprostone due to its potent uterotonic properties. Clinical trials reveal Carboprost achieves faster uterine contraction and reduced bleeding volume, making it preferable in severe cases. Dinoprostone, while effective for labor induction, shows lower efficacy in managing acute hemorrhagic conditions.
Side Effects and Safety Profiles
Carboprost commonly causes side effects such as nausea, vomiting, diarrhea, fever, and bronchospasm, with higher risk in patients with asthma or cardiovascular disease. Dinoprostone is associated with uterine hyperstimulation, fever, nausea, and vomiting, but generally has a safer profile for patients with respiratory or cardiac issues. Monitoring for uterine tachysystole and fetal distress is crucial with both drugs to ensure maternal and fetal safety during labor induction.
Administration Routes and Dosage
Carboprost is typically administered via intramuscular injection at a dosage of 250 mcg every 15 to 90 minutes, not exceeding 2 mg in 24 hours, primarily used for postpartum hemorrhage. Dinoprostone is commonly given as a vaginal insert or gel, with dosages ranging from a 10 mg vaginal insert (slow-release over 12 hours) to 0.5 mg intracervical gel, utilized for cervical ripening and labor induction. Both drugs require careful dosing adjustments based on clinical response and patient-specific factors to minimize adverse effects.
Contraindications and Precautions
Carboprost is contraindicated in patients with active cardiac, pulmonary, renal, or hepatic disease due to risks of severe bronchospasm and hypertension, while dinoprostone is contraindicated in cases of hypersensitivity, acute pelvic inflammatory disease, and unexplained vaginal bleeding. Precautions for carboprost include careful monitoring in individuals with asthma or glaucoma, whereas dinoprostone requires caution in women with uterine scarring or previous cesarean section to prevent uterine rupture. Both drugs demand vigilant assessment of maternal and fetal status to avoid adverse complications during labor induction or postpartum hemorrhage management.
Drug Interactions
Carboprost and Dinoprostone both carry risk of drug interactions primarily with other uterotonic agents, anticholinergics, and nonsteroidal anti-inflammatory drugs (NSAIDs), which may alter their efficacy or increase adverse effects such as uterine hyperstimulation. Carboprost's prostaglandin F2-alpha analog structure specifically increases the risk of interactions with vasoconstrictors and beta-agonists, potentially exacerbating cardiovascular side effects. Dinoprostone, a prostaglandin E2 analog, may have additive effects when combined with oxytocin or magnesium sulfate, necessitating careful monitoring during labor induction or abortion procedures.
Patient Selection Criteria
Carboprost is preferred for patients requiring rapid uterine contraction, especially in cases of refractory postpartum hemorrhage unresponsive to oxytocin, while dinoprostone is commonly chosen for cervical ripening and labor induction in patients with a favorable cervix or those at term with no contraindications to prostaglandins. Dinoprostone is generally safer for patients with cardiovascular or respiratory conditions due to its shorter duration of action and lower risk of bronchospasm compared to carboprost. Patient selection between these agents involves assessing uterine readiness, hemorrhage severity, and comorbidities to optimize efficacy and minimize adverse effects.
Summary and Clinical Recommendations
Carboprost and dinoprostone are prostaglandin analogs used primarily for labor induction and management of postpartum hemorrhage. Carboprost is more effective in controlling severe postpartum bleeding due to its potent uterotonic effects, while dinoprostone is preferred for cervical ripening and labor induction because of its safety profile and ease of administration. Clinical guidelines recommend carboprost for refractory hemorrhage after oxytocin failure, whereas dinoprostone is the first-line agent for cervical dilation in term pregnancies without contraindications.
Carboprost Infographic