Lytic processes play a crucial role in breaking down complex molecules into simpler components, enabling efficient nutrient recycling and energy release in biological systems. Understanding lytic activity can enhance your grasp of cellular functions and microbial interactions. Explore the rest of the article to discover how lytic mechanisms impact health and environmental cycles.
Table of Comparison
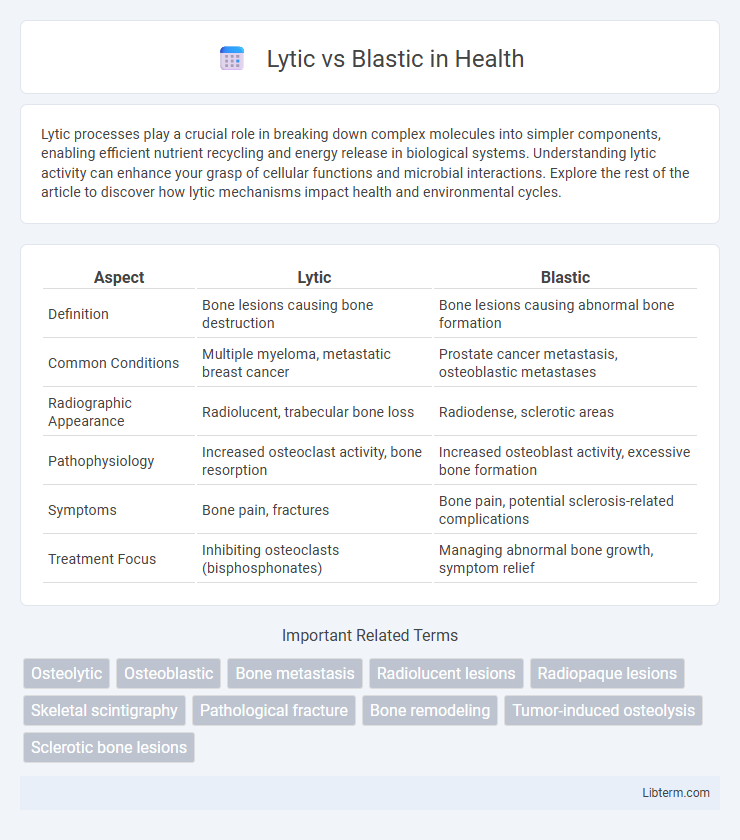
| Aspect | Lytic | Blastic |
|---|---|---|
| Definition | Bone lesions causing bone destruction | Bone lesions causing abnormal bone formation |
| Common Conditions | Multiple myeloma, metastatic breast cancer | Prostate cancer metastasis, osteoblastic metastases |
| Radiographic Appearance | Radiolucent, trabecular bone loss | Radiodense, sclerotic areas |
| Pathophysiology | Increased osteoclast activity, bone resorption | Increased osteoblast activity, excessive bone formation |
| Symptoms | Bone pain, fractures | Bone pain, potential sclerosis-related complications |
| Treatment Focus | Inhibiting osteoclasts (bisphosphonates) | Managing abnormal bone growth, symptom relief |
Introduction to Lytic and Blastic Lesions
Lytic lesions are characterized by the destruction of bone tissue resulting in areas of radiolucency on imaging, often indicating aggressive bone resorption due to malignancy or infection. Blastic lesions, in contrast, represent abnormal new bone formation manifesting as sclerotic, radiopaque regions typically associated with metastatic cancer such as prostate carcinoma. Recognizing the distinct radiographic and pathological features of lytic and blastic lesions is critical for diagnosis, prognosis, and treatment strategies in skeletal pathology.
Definitions and Core Differences
Lytic lesions refer to areas of bone destruction characterized by increased bone resorption leading to radiolucent spots on imaging, whereas blastic lesions involve abnormal bone formation resulting in sclerotic or radiopaque areas. Core differences lie in their pathological processes: lytic lesions cause bone loss often seen in metastatic cancers like multiple myeloma, while blastic lesions indicate excessive bone deposition commonly associated with prostate cancer metastases. Understanding these distinctions is crucial for accurate diagnosis, treatment planning, and prognosis in bone-related diseases.
Etiology: Causes of Lytic and Blastic Lesions
Lytic lesions primarily result from increased osteoclastic activity causing bone resorption, commonly seen in conditions like multiple myeloma, metastases from lung or thyroid cancer, and infections such as osteomyelitis. Blastic lesions arise from excessive osteoblastic activity leading to abnormal new bone formation, frequently associated with prostate cancer metastases, osteosarcoma, and Paget's disease of bone. Differentiating these lesions through imaging and clinical history aids in diagnosing underlying malignancies or metabolic bone disorders.
Common Diseases Associated with Each Type
Lytic bone lesions commonly occur in multiple myeloma, metastatic cancers such as lung and renal cell carcinoma, and hyperparathyroidism, characterized by bone destruction and increased osteoclastic activity. Blastic lesions are typically associated with prostate cancer metastases, osteosarcoma, and Paget's disease, showing abnormal bone formation and increased osteoblastic activity. Identifying the lesion type aids in diagnosing underlying diseases and tailoring appropriate treatment strategies.
Radiological Appearance: Lytic vs Blastic
Lytic lesions appear as well-defined areas of bone destruction with radiolucent qualities on X-rays, often causing cortical thinning and possible pathological fractures. Blastic lesions present as areas of increased bone density or sclerosis, showing radiopaque patches with irregular margins and increased bone formation. Radiologically, lytic lesions indicate bone resorption, while blastic lesions suggest abnormal new bone growth or osteoblastic activity.
Clinical Manifestations and Symptoms
Lytic lesions typically cause bone pain, pathological fractures, and hypercalcemia due to increased bone resorption, often seen in multiple myeloma and metastatic cancers such as lung or renal carcinoma. Blastic lesions, characterized by new bone formation, commonly present with localized bone pain and increased bone density on imaging, frequently associated with prostate cancer metastases. Both lesion types may result in neurological symptoms if there is spinal cord or nerve root compression.
Diagnostic Approaches and Tools
Lytic and blastic lesions require distinct diagnostic approaches to accurately characterize bone pathology; traditional radiography often reveals lytic lesions as areas of bone resorption with radiolucent features, while blastic lesions appear as sclerotic, radiodense regions. Advanced imaging modalities such as CT scans provide detailed bone architecture assessment, helping differentiate lytic destruction from blastic sclerosis, while MRI offers superior soft tissue contrast and marrow involvement evaluation. Bone biopsy remains the gold standard for definitive diagnosis, enabling histopathological examination to distinguish malignant lytic lesions from benign blastic growths, guiding targeted treatment strategies.
Treatment Strategies and Prognosis
Lytic bone lesions often require aggressive treatment strategies like bisphosphonates or radiation therapy to control bone destruction and alleviate pain. Blastic lesions typically respond better to hormonal therapy, chemotherapy, or targeted agents that address the underlying tumor activity and promote bone formation. Prognosis varies significantly; lytic lesions generally indicate more aggressive disease with higher fracture risk, while blastic lesions may signal a more indolent course but still require close monitoring for complications.
Lytic and Blastic Lesions in Cancer Metastasis
Lytic lesions in cancer metastasis result from tumor-induced bone resorption, characterized by the destruction of bone tissue leading to weakened skeletal structures and increased fracture risk. Blastic lesions, by contrast, involve abnormal bone formation due to osteoblastic activity stimulated by metastatic cancer cells, producing dense, sclerotic areas on imaging. Understanding the distinct mechanisms of lytic versus blastic lesions is crucial for diagnosing bone metastases and tailoring therapeutic approaches in cancers such as breast and prostate carcinoma.
Summary and Clinical Implications
Lytic bone lesions involve bone destruction caused by increased osteoclastic activity, commonly seen in multiple myeloma and metastatic cancers such as lung or renal carcinoma. Blastic bone lesions result from excessive osteoblastic activity, leading to abnormal bone formation typical of prostate cancer metastases and osteosclerotic disorders. Clinically, distinguishing between lytic and blastic lesions guides diagnosis, prognosis, and treatment strategies, with lytic lesions often causing pathological fractures and hypercalcemia, while blastic lesions may indicate increased bone pain and risk of skeletal complications.
Lytic Infographic