Hyponatremia occurs when sodium levels in the blood drop below normal, causing symptoms like nausea, headaches, confusion, and in severe cases, seizures or coma. Understanding the causes, such as excessive fluid intake or certain medical conditions, is essential for effective management and prevention. Discover how to recognize, treat, and prevent hyponatremia by exploring the detailed information in the rest of this article.
Table of Comparison
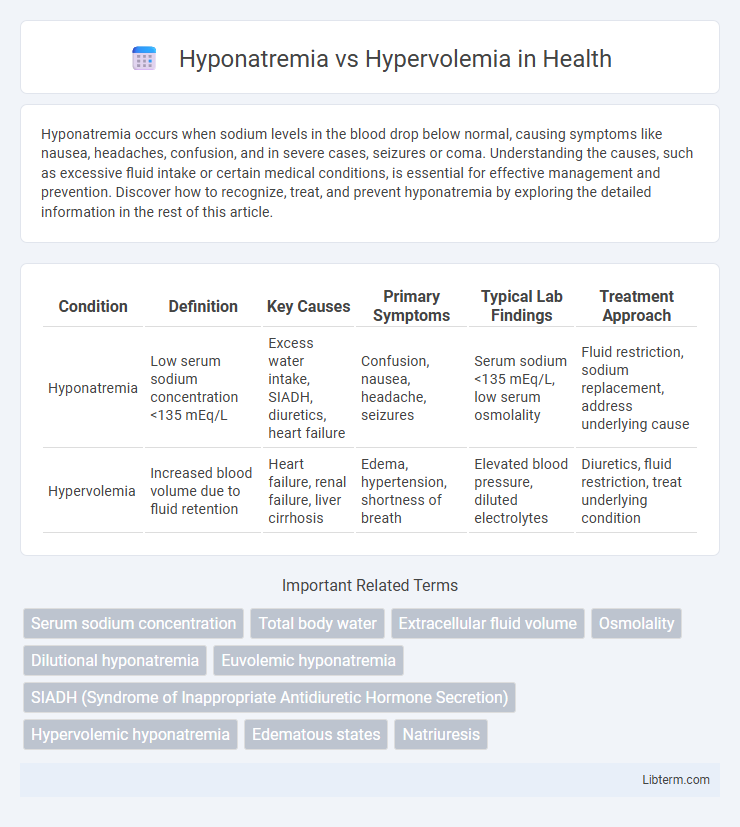
| Condition | Definition | Key Causes | Primary Symptoms | Typical Lab Findings | Treatment Approach |
|---|---|---|---|---|---|
| Hyponatremia | Low serum sodium concentration <135 mEq/L | Excess water intake, SIADH, diuretics, heart failure | Confusion, nausea, headache, seizures | Serum sodium <135 mEq/L, low serum osmolality | Fluid restriction, sodium replacement, address underlying cause |
| Hypervolemia | Increased blood volume due to fluid retention | Heart failure, renal failure, liver cirrhosis | Edema, hypertension, shortness of breath | Elevated blood pressure, diluted electrolytes | Diuretics, fluid restriction, treat underlying condition |
Introduction to Hyponatremia and Hypervolemia
Hyponatremia is a clinical condition characterized by low sodium concentration in the blood, typically below 135 mmol/L, leading to cellular swelling and neurological symptoms. Hypervolemia involves an excessive increase in blood volume often caused by heart failure, kidney disease, or liver cirrhosis, resulting in fluid overload and edema. Both disorders disrupt fluid and electrolyte balance, requiring accurate diagnosis and targeted treatment to prevent severe complications.
Definitions: Hyponatremia vs Hypervolemia
Hyponatremia is a medical condition characterized by an abnormally low concentration of sodium in the blood, typically below 135 mmol/L, leading to cellular swelling and neurological symptoms. Hypervolemia refers to an excessive increase in blood plasma volume, often caused by fluid retention due to heart, liver, or kidney conditions, resulting in edema and hypertension. Both conditions affect fluid and electrolyte balance but differ fundamentally in sodium concentration versus blood volume status.
Causes and Risk Factors
Hyponatremia often results from conditions like excessive water intake, heart failure, liver cirrhosis, or syndrome of inappropriate antidiuretic hormone secretion (SIADH), which cause diluted sodium levels in the blood. Hypervolemia is commonly caused by fluid retention due to chronic kidney disease, congestive heart failure, or liver cirrhosis, leading to increased circulating blood volume. Both conditions share risk factors such as underlying cardiovascular or renal disorders and the use of medications like diuretics or antidiuretic hormone analogs.
Pathophysiology: Mechanisms of Imbalance
Hyponatremia occurs when excessive water retention or sodium loss dilutes serum sodium levels, often due to impaired renal water excretion or inappropriate antidiuretic hormone secretion. Hypervolemia arises from increased extracellular fluid volume caused by sodium and water retention, frequently linked to heart failure, kidney disease, or cirrhosis disrupting fluid homeostasis. Both conditions involve dysregulated sodium-water balance but differ in their underlying pathophysiological mechanisms and volume status disturbances.
Clinical Manifestations and Symptoms
Hyponatremia presents with clinical manifestations such as nausea, headache, confusion, seizures, and in severe cases, coma due to the decreased serum sodium levels leading to cerebral edema. Hypervolemia is characterized by symptoms including peripheral edema, pulmonary congestion, elevated jugular venous pressure, and hypertension caused by fluid overload and increased blood volume. Differentiating these conditions requires careful evaluation of volume status and electrolyte imbalances to guide appropriate treatment.
Diagnostic Criteria and Laboratory Findings
Hyponatremia is characterized by a serum sodium concentration below 135 mEq/L, often accompanied by low serum osmolality (<275 mOsm/kg) and may present with hypovolemia, euvolemia, or hypervolemia depending on the underlying cause. Hypervolemia involves increased extracellular fluid volume with clinical signs such as edema and elevated central venous pressure, typically showing hyponatremia with low serum osmolality, but elevated urine sodium in renal salt wasting or low urine sodium in heart failure or cirrhosis. Laboratory findings for hyponatremia focus on serum sodium, serum osmolality, urine sodium concentration, and urine osmolality to differentiate volume status, while hypervolemia diagnosis relies on evidence of fluid overload through physical examination and laboratory markers like natriuretic peptides and renal function tests.
Key Differences: Hyponatremia vs Hypervolemia
Hyponatremia is characterized by low sodium concentration in the blood, typically below 135 mEq/L, often due to excessive free water retention or sodium loss. Hypervolemia involves an increase in total body sodium and water, leading to fluid overload and symptoms such as edema and hypertension. The key difference lies in hyponatremia's focus on sodium imbalance primarily affecting plasma osmolality, whereas hypervolemia centers on expanded extracellular fluid volume regardless of sodium concentration.
Treatment Approaches and Management Strategies
Hyponatremia treatment focuses on correcting sodium levels through fluid restriction, sodium supplementation, or hypertonic saline in severe cases, while carefully monitoring for osmotic demyelination syndrome. Hypervolemia management prioritizes reducing fluid overload using diuretics such as loop diuretics, sodium restriction, and addressing underlying causes like heart failure or kidney disease. Both conditions require individualized treatment plans based on patient volume status, electrolyte balance, and symptom severity to prevent complications and restore homeostasis.
Complications and Prognosis
Hyponatremia often leads to neurological complications such as cerebral edema, seizures, and altered mental status due to rapid sodium imbalance in brain cells. Hypervolemia primarily causes complications like pulmonary edema, congestive heart failure, and hypertension resulting from excess fluid accumulation and increased vascular volume. Prognosis for hyponatremia depends on the speed of correction and underlying causes, while hypervolemia prognosis is linked to managing fluid overload and cardiovascular comorbidities.
Prevention and Monitoring Strategies
Effective prevention of hyponatremia involves careful regulation of fluid intake and monitoring of sodium levels in at-risk patients, particularly those with heart failure or renal impairment. Hypervolemia prevention focuses on controlling dietary sodium and implementing diuretic therapy under clinical supervision to avoid fluid overload. Regular assessment of electrolyte balance, body weight, and vital signs facilitates early detection and management of both conditions, reducing the risk of complications.
Hyponatremia Infographic