Anuria is a medical condition characterized by the absence of urine output, often signaling severe kidney dysfunction or urinary tract obstruction. Prompt diagnosis and treatment are crucial to prevent life-threatening complications such as electrolyte imbalances and fluid overload. Explore the rest of the article to understand the causes, symptoms, and treatment options for anuria to safeguard your health.
Table of Comparison
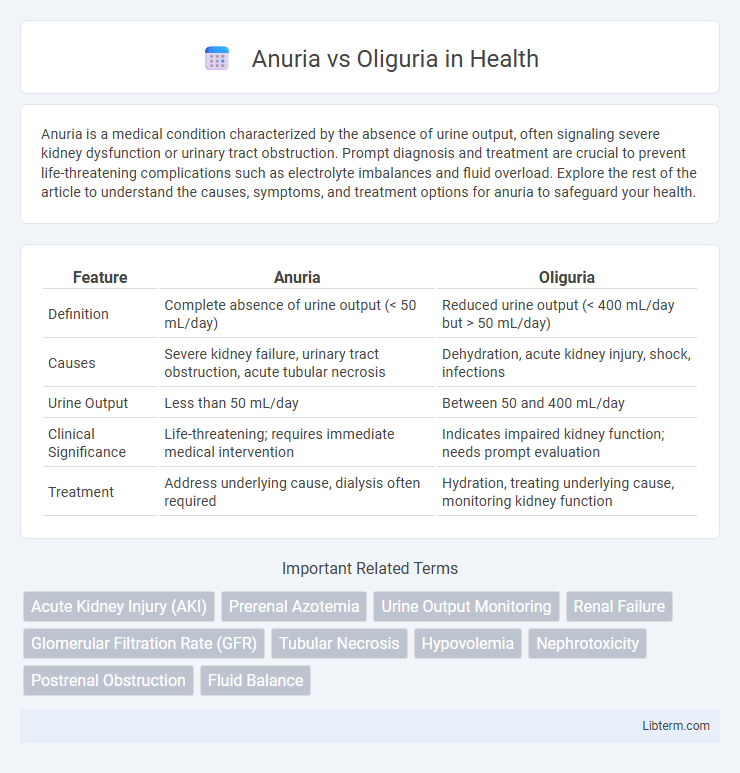
| Feature | Anuria | Oliguria |
|---|---|---|
| Definition | Complete absence of urine output (< 50 mL/day) | Reduced urine output (< 400 mL/day but > 50 mL/day) |
| Causes | Severe kidney failure, urinary tract obstruction, acute tubular necrosis | Dehydration, acute kidney injury, shock, infections |
| Urine Output | Less than 50 mL/day | Between 50 and 400 mL/day |
| Clinical Significance | Life-threatening; requires immediate medical intervention | Indicates impaired kidney function; needs prompt evaluation |
| Treatment | Address underlying cause, dialysis often required | Hydration, treating underlying cause, monitoring kidney function |
Introduction to Anuria and Oliguria
Anuria is a medical condition characterized by the absence of urine production, typically defined as less than 50 milliliters per day, indicating severe kidney dysfunction or urinary obstruction. Oliguria refers to a significantly reduced urine output, generally less than 400 milliliters per day, often signaling acute kidney injury, dehydration, or systemic illness. Both conditions are critical indicators in nephrology, requiring prompt diagnosis to prevent irreversible renal damage and ensure appropriate treatment.
Definitions: Anuria vs Oliguria
Anuria is defined as a urinary output of less than 100 milliliters per day, indicating severe kidney failure or obstruction. Oliguria refers to a reduced urine output, typically less than 400 milliliters per day, signaling impaired renal function or dehydration. Both conditions serve as critical indicators in diagnosing acute kidney injury and require prompt medical evaluation.
Common Causes of Anuria
Anuria, characterized by urine output less than 50 mL per day, commonly results from acute kidney injury, bilateral ureteral obstruction, or severe dehydration leading to renal hypoperfusion. In contrast, oliguria is defined by reduced urine output between 100-400 mL per day and often indicates early-stage kidney dysfunction or volume depletion. Understanding the common causes of anuria, such as acute tubular necrosis, urinary tract obstruction, and prerenal azotemia, is crucial for timely diagnosis and intervention.
Common Causes of Oliguria
Oliguria, defined as urine output less than 400 mL per day in adults, commonly results from conditions such as acute kidney injury, dehydration, heart failure, or urinary tract obstruction. In contrast, anuria is characterized by urine output less than 100 mL per day and usually indicates severe renal failure or complete urinary tract obstruction. Identifying the underlying causes of oliguria is crucial for timely intervention and preventing progression to anuria.
Pathophysiological Differences
Anuria is characterized by the complete cessation of urine production, often resulting from severe acute kidney injury or obstruction causing a near-total loss of glomerular filtration rate. Oliguria involves reduced urine output, typically less than 400 mL per day, reflecting partial impairment in renal perfusion or tubular function. The pathophysiological differences hinge on the extent of nephron damage and functional capacity, with anuria indicating more profound tubular necrosis or obstruction compared to the milder ischemic or prerenal causes underlying oliguria.
Clinical Manifestations
Anuria is characterized by a complete absence of urine production, often indicating severe kidney failure or urinary tract obstruction, while oliguria is defined by low urine output, typically less than 400 mL per day, suggesting acute kidney injury or dehydration. Clinical manifestations of anuria include fluid overload, hypertension, and electrolyte imbalances, whereas oliguria presents with signs of decreased renal perfusion, such as low blood pressure, dry mucous membranes, and decreased skin turgor. Both conditions require prompt evaluation of renal function tests, serum electrolytes, and urinalysis to determine the underlying etiology and guide treatment.
Diagnostic Criteria and Assessment
Anuria is defined by a urine output of less than 50 mL per day, indicating nearly complete renal failure, while oliguria is characterized by urine output between 100 to 400 mL per day, signaling significant but partial reduction in kidney function. Diagnostic criteria for anuria involve identifying causes like bilateral urinary tract obstruction or acute tubular necrosis through imaging and serum creatinine levels, whereas oliguria assessment includes evaluating volume status, estimating glomerular filtration rate (GFR), and monitoring electrolyte imbalances. Accurate differentiation is critical for timely intervention, with urine output measurement, fractional excretion of sodium (FENa), and blood urea nitrogen (BUN) to creatinine ratio serving as key diagnostic tools in clinical settings.
Treatment Approaches and Management
Anuria, characterized by urine output less than 100 mL/day, requires urgent interventions such as dialysis or aggressive fluid management to prevent life-threatening complications, while oliguria, defined by urine output between 100 and 400 mL/day, often responds to addressing underlying causes like dehydration or acute kidney injury through intravenous fluids or diuretics. Treatment for both conditions involves careful monitoring of electrolytes, hemodynamic status, and renal function parameters to guide therapy and prevent progression to chronic kidney disease. Early identification and targeted management of these distinct but related conditions improve patient outcomes by restoring adequate renal perfusion and minimizing renal tissue damage.
Prognosis and Complications
Anuria, defined as urine output less than 50 mL per day, generally indicates severe renal failure with a poorer prognosis compared to oliguria, which involves urine output between 50 and 400 mL per day. Complications of anuria often include electrolyte imbalances, fluid overload, and uremic toxicity, significantly increasing the risk of morbidity and mortality. Oliguria, while less severe, can progress to anuria if untreated and may lead to acute kidney injury, requiring timely intervention to prevent irreversible renal damage.
Prevention and Patient Education
Preventing anuria and oliguria involves maintaining adequate hydration, monitoring kidney function regularly, and managing underlying conditions such as diabetes or hypertension that contribute to renal impairment. Patient education should emphasize recognizing early signs of decreased urine output, the importance of adhering to prescribed medications, and lifestyle modifications like reducing salt intake and avoiding nephrotoxic substances. Promoting timely medical consultation for symptoms like swelling, fatigue, or confusion can help prevent progression to severe kidney failure.
Anuria Infographic